

Prevalence of Hypertension in Children with Early-Stage ADPKD
- PMID: 29674338
- PMCID: PMC5989684
- DOI: 10.2215/CJN.11401017
Prevalence of Hypertension in Children with Early-Stage ADPKD
Abstract
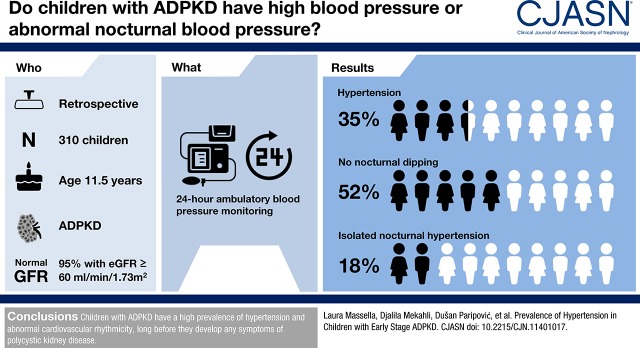
Background and objectives: Autosomal dominant polycystic kidney disease is the most common inheritable kidney disease, frequently thought to become symptomatic in adulthood. However, patients with autosomal dominant polycystic kidney disease may develop signs or symptoms during childhood, in particular hypertension. Although ambulatory BP monitoring is the preferred method to diagnose hypertension in pediatrics, data in children with autosomal dominant polycystic kidney disease are limited.
Design, setting, participants, & measurements: Our retrospective multicenter study was conducted to collect ambulatory BP monitoring recordings from patients with autosomal dominant polycystic kidney disease age <18 years old. Basic anthropometric parameters as well as data on kidney function, BP treatment, and kidney ultrasound were also collected.
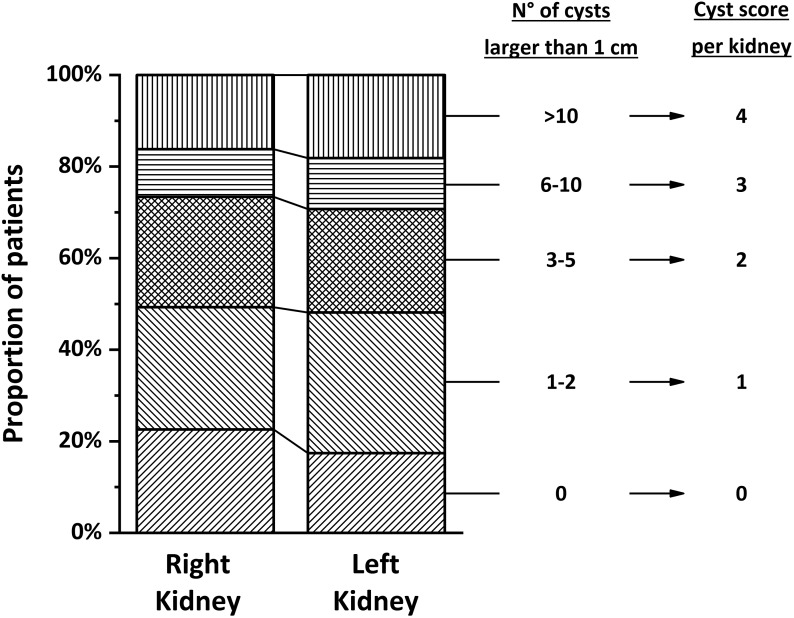
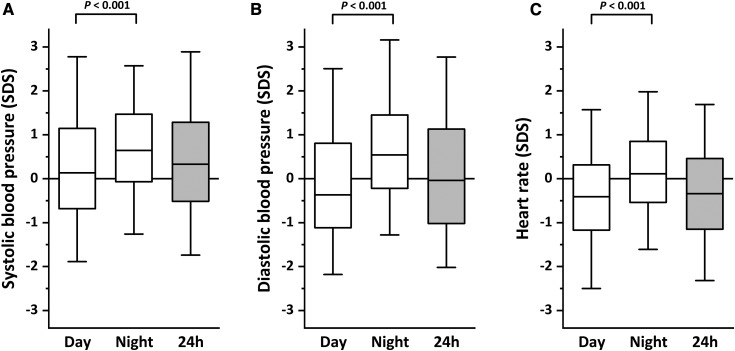
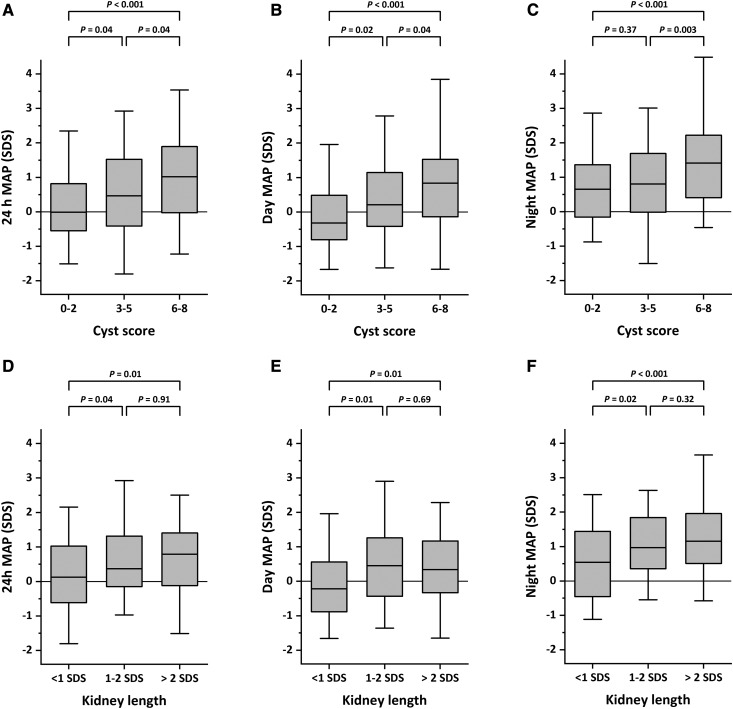
Results: Data from 310 children with autosomal dominant polycystic kidney disease with a mean age of 11.5±4.1 years old were collected at 22 European centers. At the time when ambulatory BP monitoring was performed, 95% of children had normal kidney function. Reference data for ambulatory BP monitoring were available for 292 patients. The prevalence rates of children with hypertension and/or those who were treated with antihypertensive drugs were 31%, 42%, and 35% during daytime, nighttime, or the entire 24-hour cycle, respectively. In addition, 52% of participants lacked a physiologic nocturnal BP dipping, and 18% had isolated nocturnal hypertension. Logistic regression analysis showed a significant association between a categorical cyst score that was calculated on the basis of the number of cysts >1 cm per kidney and daytime hypertension (odds ratio, 1.70; 95% confidence interval, 1.21 to 2.4; P=0.002), nighttime hypertension (odds ratio, 1.31; 95% confidence interval, 1.05 to 1.63; P=0.02), or 24-hour hypertension (odds ratio, 1.39; 95% confidence interval, 1.08 to 1.81; P=0.01). Kidney length, expressed as SD score, was also significantly associated with nighttime hypertension (odds ratio, 1.23; 95% confidence interval, 1.06 to 1.42; P=0.10).
Conclusions: These data indicate high prevalence of hypertension in children with autosomal dominant polycystic kidney disease starting at young ages.
Keywords: ABPM; Ambulatory Blood Pressure Monitoring; Antihypertensive Agents; Autosomal Dominant Polycystic Kidney Disease; Blood Pressure Determination; Blood Pressure Monitoring, Ambulatory; Child; Cysts; Humans; Logistic Models; Polycystic Kidney, Autosomal Dominant; Prevalence; Retrospective Studies; Rhythm Analysis; blood pressure; hypertension; kidney; pediatrics.
Copyright © 2018 by the American Society of Nephrology.
Figures
References
-
- Ong AC, Devuyst O, Knebelmann B, Walz G; ERA-EDTA Working Group for Inherited Kidney Diseases : Autosomal dominant polycystic kidney disease: The changing face of clinical management. Lancet 385: 1993–2002, 2015 - PubMed
-
- Selistre L, de Souza V, Ranchin B, Hadj-Aissa A, Cochat P, Dubourg L: Early renal abnormalities in children with postnatally diagnosed autosomal dominant polycystic kidney disease. Pediatr Nephrol 27: 1589–1593, 2012 - PubMed
-
- Seeman T, Dusek J, Vondrichová H, Kyncl M, John U, Misselwitz J, Janda J: Ambulatory blood pressure correlates with renal volume and number of renal cysts in children with autosomal dominant polycystic kidney disease. Blood Press Monit 8: 107–110, 2003 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
