

Children with cerebral malaria or severe malarial anaemia lack immunity to distinct variant surface antigen subsets
- PMID: 29674705
- PMCID: PMC5908851
- DOI: 10.1038/s41598-018-24462-4
Children with cerebral malaria or severe malarial anaemia lack immunity to distinct variant surface antigen subsets
Abstract
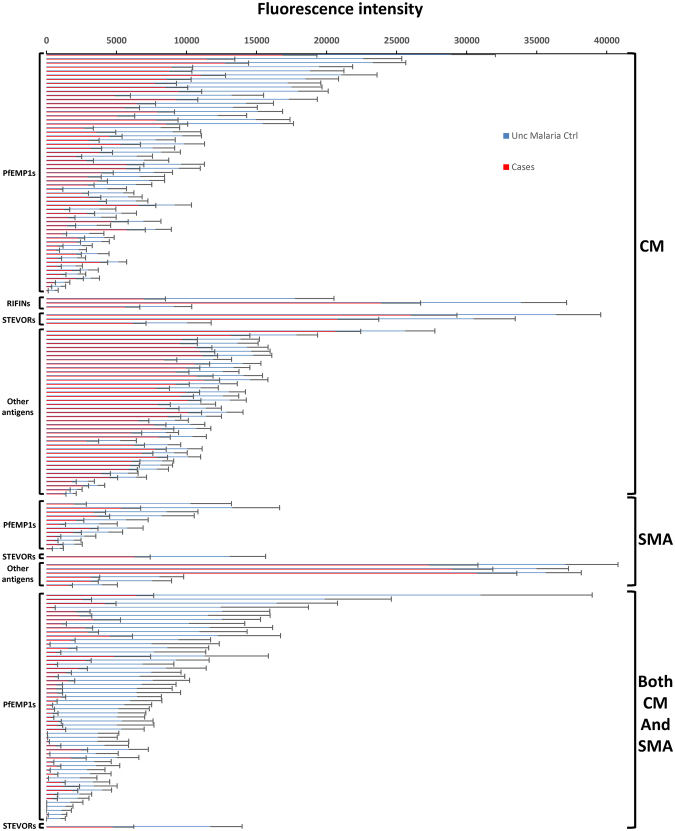
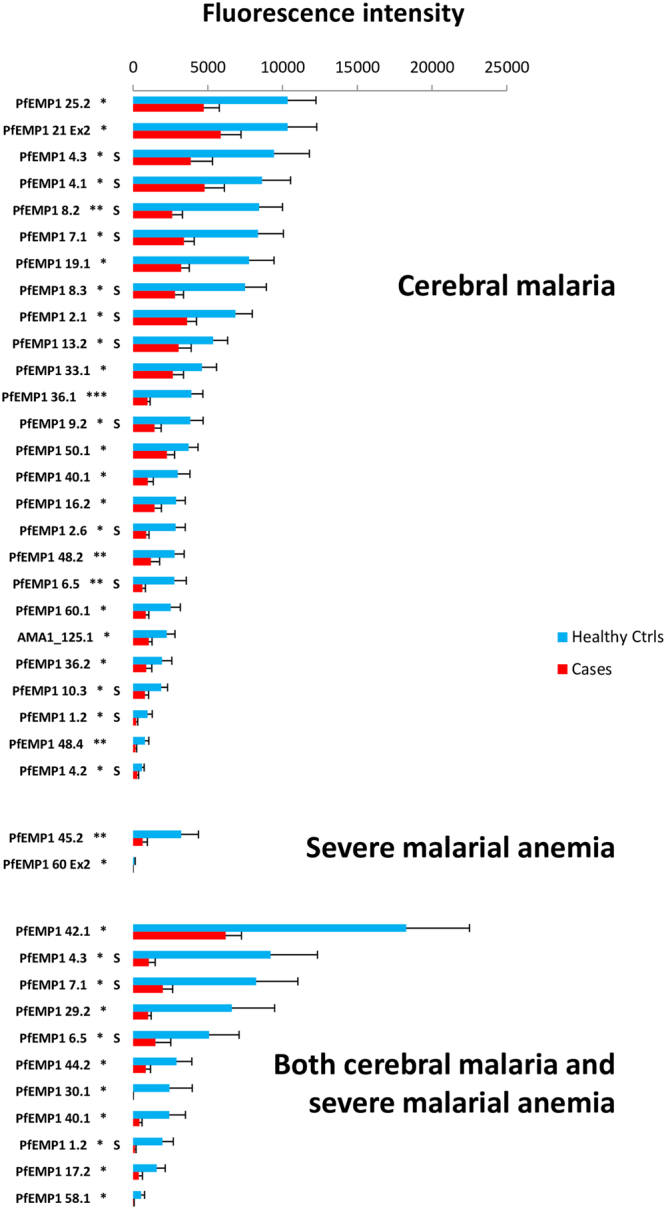
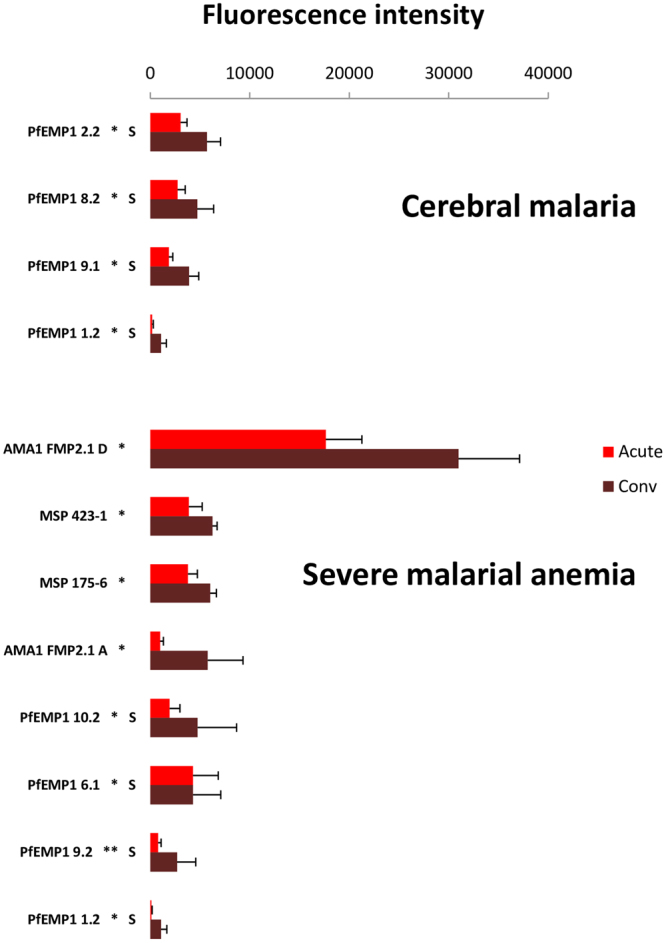
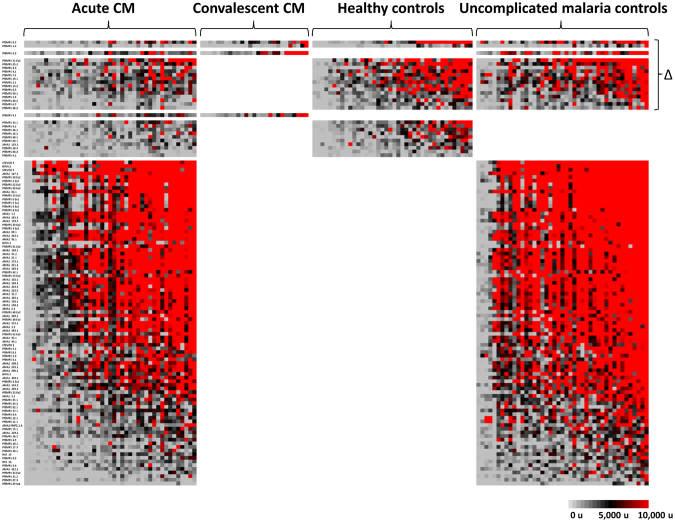
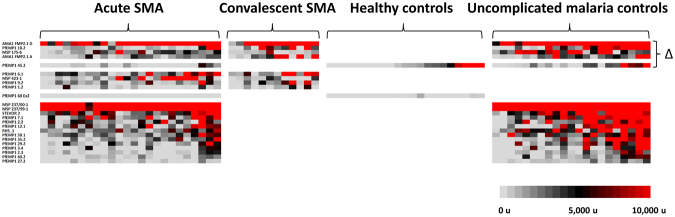
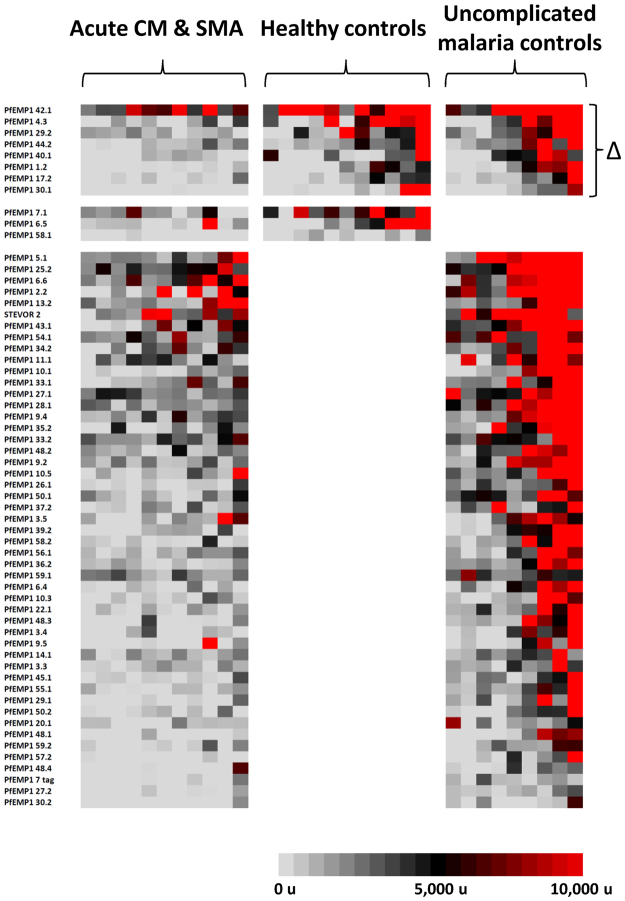
Variant surface antigens (VSAs) play a critical role in severe malaria pathogenesis. Defining gaps, or "lacunae", in immunity to these Plasmodium falciparum antigens in children with severe malaria would improve our understanding of vulnerability to severe malaria and how protective immunity develops. Using a protein microarray with 179 antigen variants from three VSA families as well as more than 300 variants of three other blood stage P. falciparum antigens, reactivity was measured in sera from Malian children with cerebral malaria or severe malarial anaemia and age-matched controls. Sera from children with severe malaria recognized fewer extracellular PfEMP1 fragments and were less reactive to specific fragments compared to controls. Following recovery from severe malaria, convalescent sera had increased reactivity to certain non-CD36 binding PfEMP1s, but not other malaria antigens. Sera from children with severe malarial anaemia reacted to fewer VSAs than did sera from children with cerebral malaria, and both of these groups had lacunae in their seroreactivity profiles in common with children who had both cerebral malaria and severe malarial anaemia. This microarray-based approach may identify a subset of VSAs that could inform the development of a vaccine to prevent severe disease or a diagnostic test to predict at-risk children.
Conflict of interest statement
P.L.F. holds patents related to technology applied in this study and has stock positions with Antigen Discovery.
Figures

Similar articles
-
Plasmodium falciparum variant surface antigen expression varies between isolates causing severe and nonsevere malaria and is modified by acquired immunity.J Immunol. 2002 Apr 1;168(7):3444-50. doi: 10.4049/jimmunol.168.7.3444. J Immunol. 2002. PMID: 11907103
-
Convalescent Plasmodium falciparum-specific seroreactivity does not correlate with paediatric malaria severity or Plasmodium antigen exposure.Malar J. 2018 Apr 25;17(1):178. doi: 10.1186/s12936-018-2323-4. Malar J. 2018. PMID: 29695240 Free PMC article.
-
Determinants of variant surface antigen antibody response in severe Plasmodium falciparum malaria in an area of low and unstable malaria transmission.Scand J Immunol. 2006 Mar;63(3):232-40. doi: 10.1111/j.1365-3083.2006.01732.x. Scand J Immunol. 2006. PMID: 16499577
-
Cerebral Plasmodium falciparum malaria: The role of PfEMP1 in its pathogenesis and immunity, and PfEMP1-based vaccines to prevent it.Immunol Rev. 2020 Jan;293(1):230-252. doi: 10.1111/imr.12807. Epub 2019 Sep 27. Immunol Rev. 2020. PMID: 31562653 Free PMC article. Review.
-
Clinical and parasitological studies on immunity to Plasmodium falciparum malaria in children.Scand J Infect Dis Suppl. 1996;102:1-53. Scand J Infect Dis Suppl. 1996. PMID: 9060051 Review.
Cited by
-
Protein Microarrays as a Tool to Analyze Antibody Responses to Variant Surface Antigens Expressed on the Surface of Plasmodium falciparum-Infected Erythrocytes.Methods Mol Biol. 2022;2470:343-358. doi: 10.1007/978-1-0716-2189-9_25. Methods Mol Biol. 2022. PMID: 35881357
-
Distinct Antibody Signatures Associated with Different Malaria Transmission Intensities in Zambia and Zimbabwe.mSphere. 2019 Mar 27;4(2):e00061-19. doi: 10.1128/mSphereDirect.00061-19. mSphere. 2019. PMID: 30918058 Free PMC article.
-
Clinico-epidemiological profiles & outcome of severe malaria in children under-five in the tribal area of Kalahandi, Odisha.Indian J Med Res. 2024 Jan 1;159(1):17-25. doi: 10.4103/ijmr.ijmr_3302_21. Epub 2024 Mar 4. Indian J Med Res. 2024. PMID: 38439122 Free PMC article.
-
IgG and IgM responses to the Plasmodium falciparum asexual stage antigens reflect respectively protection against malaria during pregnancy and infanthood.Malar J. 2024 May 19;23(1):154. doi: 10.1186/s12936-024-04970-7. Malar J. 2024. PMID: 38764069 Free PMC article.
-
Identifying Targets of Protective Antibodies against Severe Malaria in Papua, Indonesia, Using Locally Expressed Domains of Plasmodium falciparum Erythrocyte Membrane Protein 1.Infect Immun. 2022 Feb 17;90(2):e0043521. doi: 10.1128/IAI.00435-21. Epub 2021 Dec 6. Infect Immun. 2022. PMID: 34871039 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
