

Costs of medication in older patients: before and after comprehensive geriatric assessment
- PMID: 29674846
- PMCID: PMC5898882
- DOI: 10.2147/CIA.S159966
Costs of medication in older patients: before and after comprehensive geriatric assessment
Abstract
Background: Polypharmacy and inappropriate drug use cause numerous complications, such as cognitive impairment, frailty, falls, and functional dependence. The present study aimed to determine the effect of the comprehensive geriatric assessment (CGA) on polypharmacy, potentially inappropriate medications (PIMs) and potential prescribing omissions (PPOs), and to evaluate the economic reflections of medication changes.
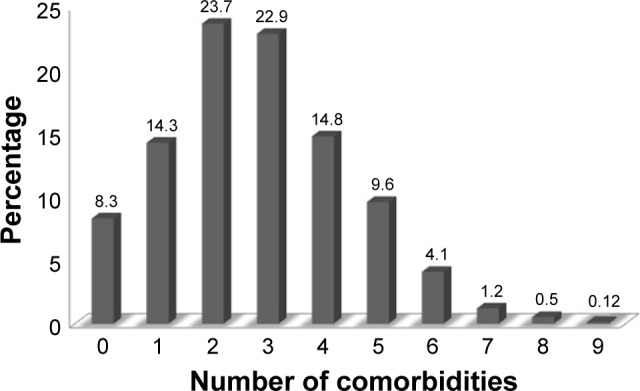
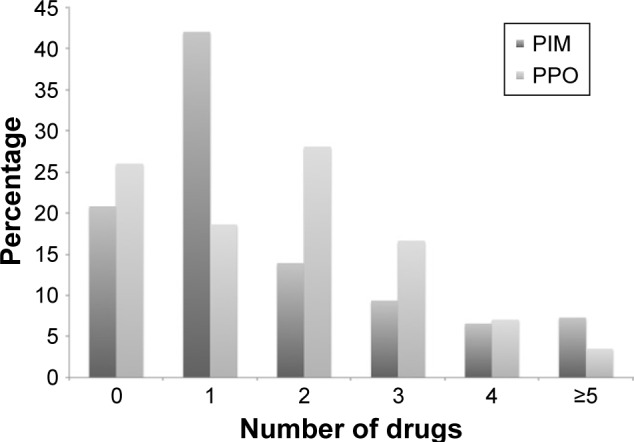
Methods: One thousand five hundred and seventy-nine older patients, who had undergone CGA, were retrospectively evaluated. The drugs, drug groups, and number of drugs that the patients used were recorded. Appropriate drug therapy was identified by both CGA and STOPP/START criteria. Based on these criteria, PIMs were discontinued and PPOs were started. The monthly cost of these drugs was calculated separately for PIMs and PPOs by using the drugstore records.
Results: After CGA, while the prevalence of non-polypharmacy was increased from 43.3% to 65.6%, the prevalence of polypharmacy and hyperpolypharmacy was decreased from 56.7% to 34.4% and 12.0% to 3.6%, respectively. The three most common PIMs discontinued were proton pump inhibitors, anti-dementia drugs, and antipsychotics, respectively. However, the most common PPOs started were vitamin D and B12 supplements, and anti-depressants. After CGA, monthly saved total per capita cost of PIMs was US$12.8 and monthly increased total per capita cost of PPOs was $5.6.
Conclusion: It was demonstrated that prevalence of polypharmacy, PIM, and PPO could be decreased by CGA including START/STOPP criteria in older adults. Furthermore, this will have beneficial effects on economical parameters due to decreasing drug-related health care costs.
Keywords: comprehensive geriatric assessment; cost; elderly; polypharmacy.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
Comment on
-
Dementia-Related Results of "Costs of Medication in Older Patients: Before and After Comprehensive Geriatric Assessment".Am J Alzheimers Dis Other Demen. 2018 Dec;33(8):497-499. doi: 10.1177/1533317518802434. Epub 2018 Sep 24. Am J Alzheimers Dis Other Demen. 2018. PMID: 30249114 Free PMC article.
References
-
- World Health Organization . World Health Statistics, 2013. Geneva: World Health Organization; Available from: http://www.who.int/gho/publications/world_health_statistics/2013/en/
-
- Wilson M, Mair A, Dreischulte T, Witham MD, NHS Scotland Model of Care Polypharmacy Working Group Prescribing to fit the needs of older people the – NHS Scotland Polypharmacy Guidance. J R Coll Physicians Edinb. (2nd edition) 2015;45(2):108–113. - PubMed
-
- Onder G, Landi F, Fusco D, et al. Recommendations to prescribe in complex older adults: results of the CRIteria to assess appropriate Medication use among Elderly complex patients (CRIME) project. Drugs Aging. 2014;31(1):33–45. - PubMed
-
- Johnson JA, Bootman JL. Drug-related morbidity and mortality. A cost-of-illness model. Arch Intern Med. 1995;155(18):1949–1956. - PubMed
-
- Ernst FR, Grizzle AJ. Drug-related morbidity and mortality: updating the cost-of-illness model. J Am Pharm Assoc (Wash) 2001;41(2):192–199. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
