

Factors affecting mortality and reoperations in high-energy pelvic fractures
- PMID: 29675632
- PMCID: PMC6132923
- DOI: 10.1007/s00590-018-2203-1
Factors affecting mortality and reoperations in high-energy pelvic fractures
Abstract
Aim: Factors affecting mortality during the first year following high-energy pelvic fractures has not been reported previously. Nor has surgical complications leading to reoperations been reported in a cohort with only high-energy pelvic trauma patients.
Objectives: The aim of this study was to report and analyse factors affecting outcome, in terms of mortality and reoperations, up to 1 year after the injury in patients with a traumatic pelvic ring injury due to a high-energy trauma.
Materials and methods: Data from the SweTrau (Swedish National Trauma Registry) on patients admitted to the Trauma Centre Karolinska in Stockholm, Sweden, were collected. Inclusion criteria were adults (age ≥ 18), trauma with a high-energy mechanism, alive on arrival, Swedish personal identification number, reported pelvic fracture on CT scan. Patient records and radiographies were reviewed. The study period was 2011-2015 with 1-year follow-up time. Univariate and regression analysis on factors affecting mortality was performed. Risk of reoperation was analysed using univariate and case-by-case analysis.
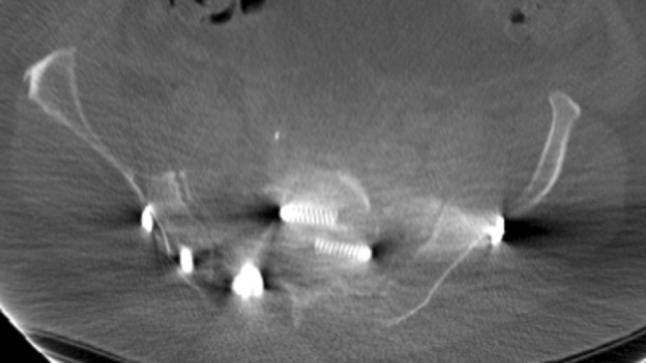
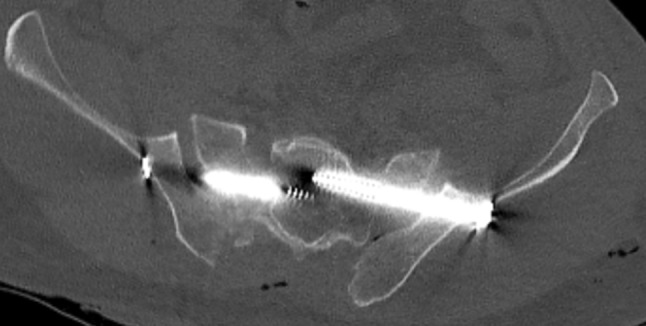
Results: We included 385 cases with mean age 47.5 ± 20.6 years (38% females): 317 pelvic fractures, 48 acetabular fractures and 20 combined injuries. Thirty-day mortality was 8% (30/385), and 1-year mortality was 9% (36/385). The main cause of death at 1 year was traumatic brain injury (14/36) followed by high age (> 70) with extensive comorbidities (8/36). Intentional fall from high altitude (OR 6, CI 2-17), GCS < 8 (OR 12, CI 5-33) and age > 70 (OR 17, CI 6-51) were factors predicting mortality. Thirty patients (22%, 30/134) were further reoperated due to hardware-related (n = 18) or non-hardware-related complications (n = 12). Hardware-related complications included: mal-placed screws (n = 7), mal-placed plate (n = 1), implant failure (n = 6), or mechanical irritation from the implant (n = 4). Non-hardware-related reasons for reoperations were: infection (n = 10), skin necrosis (n = 1), or THR due to post-traumatic osteoarthritis (n = 1).
Conclusion: Non-survivors in our study died mainly because of traumatic brain injury or high age with extensive comorbidities. Most of the mortalities occurred early. Intentional injuries and especially intentional falls from high altitude had high mortality rate. Reoperation frequency was high, and several of the hardware-related complications could potentially have been avoided.
Keywords: Accidents/mortality; Glasgow coma scale; Injury severity score; Intention; Orthopaedic surgery; Pelvic bone; Reoperation.
Conflict of interest statement
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The study was performed according to the Declaration of Helsinki and approved by the Local Ethics Committee (DNR: 2016/383-31/4).
Figures

References
-
- Melton LJ, 3rd, Sampson JM, Morrey BF, Ilstrup DM. Epidemiologic features of pelvic fractures. Clin Orthop Relat Res. 1981;155:43–47. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
