

Treatment Intensification in Type 2 Diabetes: A Real-World Study of 2-OAD Regimens, GLP-1 RAs, or Basal Insulin
- PMID: 29675797
- PMCID: PMC5984932
- DOI: 10.1007/s13300-018-0429-x
Treatment Intensification in Type 2 Diabetes: A Real-World Study of 2-OAD Regimens, GLP-1 RAs, or Basal Insulin
Abstract
Introduction: Treatment guidelines recommend a stepwise approach to glycemia management in patients with type 2 diabetes (T2D), but this may result in uncontrolled glycated hemoglobin A1c (HbA1c) between steps. This retrospective analysis compared clinical and economic outcomes among patients with uncontrolled T2D initiating two oral antidiabetes drugs (OADs), glucagon-like peptide-1 receptor agonists (GLP-1 RAs), or basal insulin in a real-world setting.
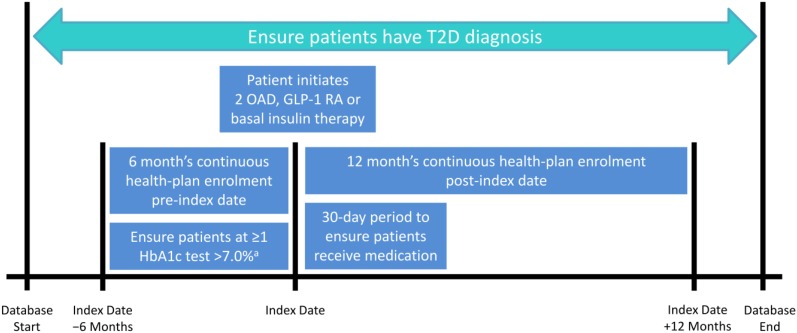
Methods: Adults with T2D on OAD monotherapy were identified in the MarketScan claims database (2007-2014). Those initiating two OADs (simultaneously or sequentially), GLP-1 RAs, or basal insulin were selected (date of initiation was termed the 'index date'); patients were required to have HbA1c > 7.0% in the 6 months pre-index date. HbA1c was compared from 6 months pre- to 1-year post-index. Annual all-cause healthcare utilization and costs were reported over the 1-year follow-up period.
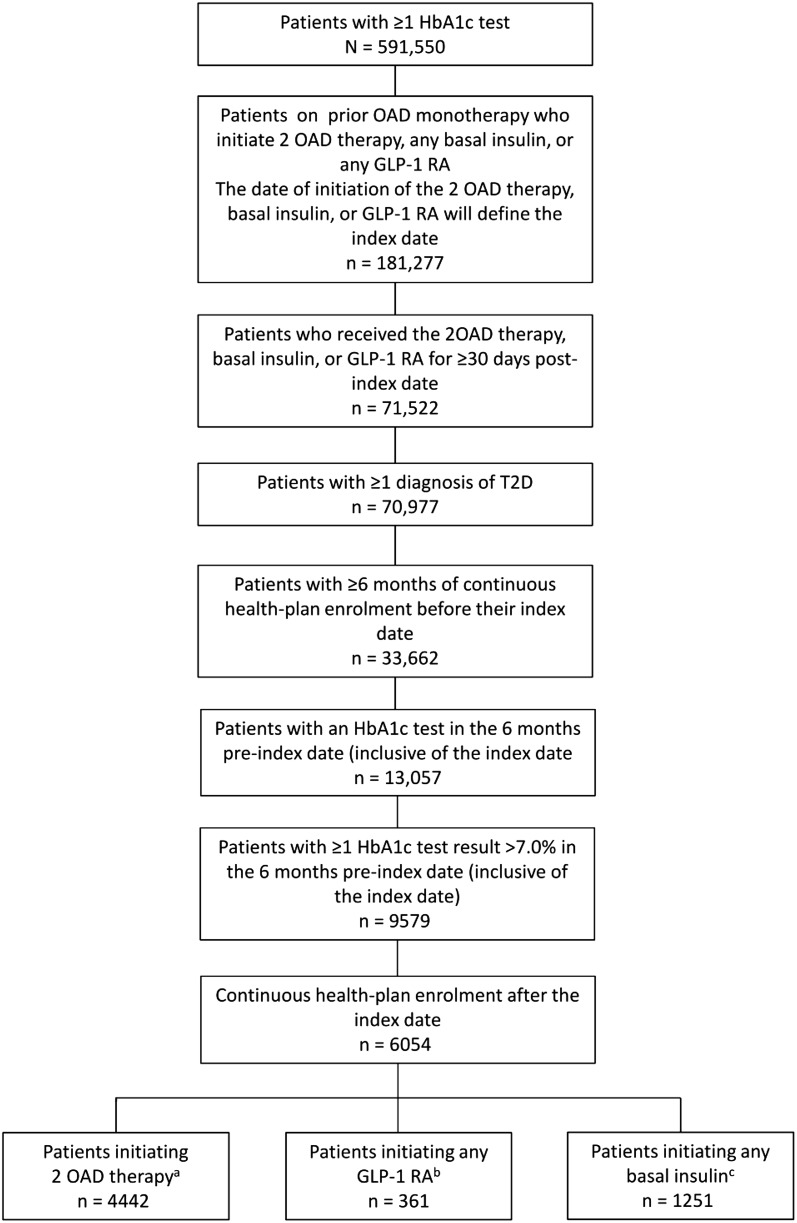
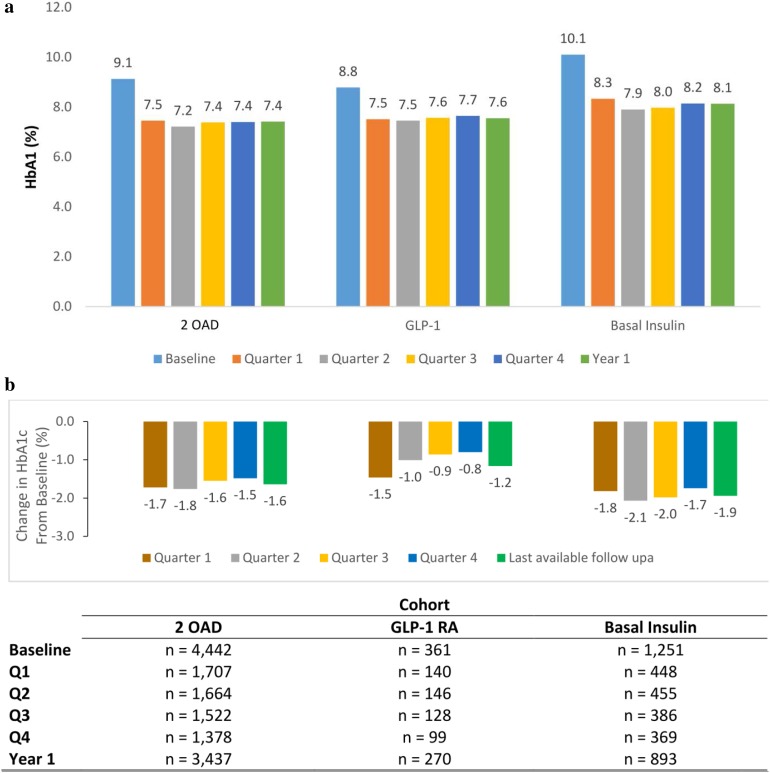
Results: Data for 6054 patients were analyzed (2-OAD, n = 4442; GLP-1 RA, n = 361; basal insulin, n = 1251). Baseline HbA1c was high in all cohorts, but highest in the basal-insulin cohort. Treatment initiation resulted in reductions in HbA1c in all cohorts, which was generally maintained throughout the follow-up period. Average HbA1c reductions from the 6 months pre- to 1 year post-index date were -1.2% for GLP-1 RA, -1.6% for OADs, and -1.8% for basal insulin. HbA1c < 7.0% at 1 year occurred in 32.6%, 47.5%, and 41.1% of patients, respectively. Annual healthcare costs (mean [SD]) were lowest for OAD (US$10,074 [$22,276]) followed by GLP-1 RA (US$14,052 [$23,829]) and basal insulin (US$18,813 [$37,332]).
Conclusion: Despite robust HbA1c lowering following treatment initiation, many patients did not achieve HbA1c < 7.0%. Basal insulin, generally prescribed for patients with high baseline HbA1c, was associated with a large reduction in HbA1c and with higher costs. Therapy intensification at an appropriate time could lead to clinical and economic benefits and should be investigated further.
Funding: Sanofi U.S., Inc.
Keywords: Basal insulin; Clinical inertia; GLP-1 RA; Oral antidiabetes drugs; Treatment intensification; Type 2 diabetes.
Figures
References
-
- American Diabetes Association Standards of medical care in diabetes—2017. Diabetes Care. 2017;40(Suppl. 1):S1–S135.
-
- Garber AJ, Abrahamson MJ, Barzilay JI, et al. Consensus statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the comprehensive type 2 diabetes management algorithm—2017 executive summary. Endocr Pract. 2017;23:207–238. doi: 10.4158/EP161682.CS. - DOI - PubMed
-
- Brown JB, Nichols GA. Slow response to loss of glycemic control in type 2 diabetes mellitus. Am J Manag Care. 2003;9:213–217. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
