

Allergen-Specific Immunotherapies for Food Allergy
- PMID: 29676066
- PMCID: PMC5911438
- DOI: 10.4168/aair.2018.10.3.189
Allergen-Specific Immunotherapies for Food Allergy
Abstract
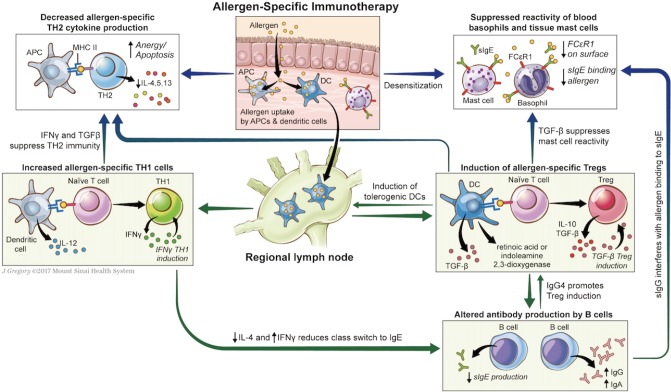
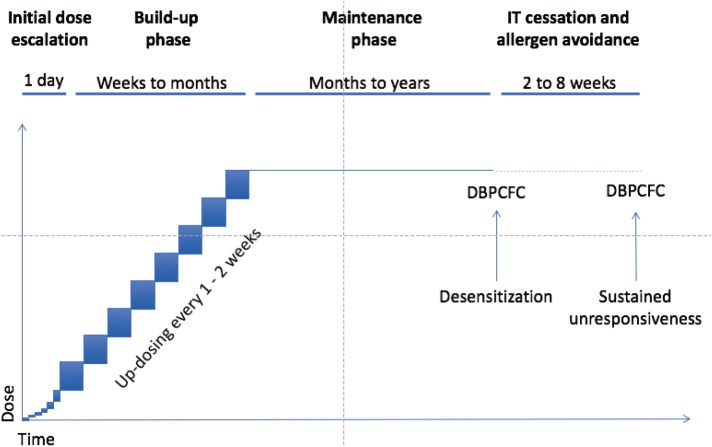
With rising prevalence of food allergy (FA), allergen-specific immunotherapy (AIT) for FA has become an active area of research in recent years. In AIT, incrementally increasing doses of inciting allergen are given with the goal to increase tolerance, initially through desensitization, which relies on regular exposure to allergen. With prolonged therapy in some subjects, AIT may induce sustained unresponsiveness, in which tolerance is retained after a period of allergen avoidance. Methods of AIT currently under study in humans include oral, sublingual, epicutaneous, and subcutaneous delivery of modified allergenic protein, as well as via DNA-based vaccines encoding allergen with lysosomal-associated membrane protein I. The balance of safety and efficacy varies by type of AIT, as well as by targeted allergen. Age, degree of sensitization, and other comorbidities may affect this balance within an individual patient. More recently, AIT with modified proteins or combined with immunomodulatory therapies has shown promise in making AIT safer and/or more effective. Though methods of AIT are neither currently advised by experts (oral immunotherapy [OIT]) nor widely available, AIT is likely to become a part of recommended management of FA in the coming years. Here, we review and compare methods of AIT currently under study in humans to prepare the practitioner for an exciting new phase in the care of food allergic patients in which improved tolerance to inciting foods will be a real possibility.
Keywords: Food allergy; epicutaneous immunotherapy; oral immunotherapy; subcutaneous immunotherapy; sublingual immunotherapy.
Copyright © 2018 The Korean Academy of Asthma, Allergy and Clinical Immunology · The Korean Academy of Pediatric Allergy and Respiratory Disease.
Conflict of interest statement
There are no financial or other issues that might lead to conflict of interest.
Figures
References
-
- Nwaru BI, Hickstein L, Panesar SS, Roberts G, Muraro A, Sheikh A, et al. Prevalence of common food allergies in Europe: a systematic review and meta-analysis. Allergy. 2014;69:992–1007. - PubMed
-
- Branum AM, Lukacs SL. Food allergy among children in the United States. Pediatrics. 2009;124:1549–1555. - PubMed
-
- Sicherer SH, Muñoz-Furlong A, Godbold JH, Sampson HA. US prevalence of self-reported peanut, tree nut, and sesame allergy: 11-year follow-up. J Allergy Clin Immunol. 2010;125:1322–1326. - PubMed
-
- Sampson HA, Aceves S, Bock SA, James J, Jones S, Lang D, et al. Food allergy: a practice parameter update-2014. J Allergy Clin Immunol. 2014;134:1016–1025.e43. - PubMed
-
- Gupta RS, Springston EE, Warrier MR, Smith B, Kumar R, Pongracic J, et al. The prevalence, severity, and distribution of childhood food allergy in the United States. Pediatrics. 2011;128:e9–e17. - PubMed
