

Bilateral herpes simplex keratitis reactivation after lacrimal gland botulinum toxin injection
- PMID: 29676321
- PMCID: PMC5939169
- DOI: 10.4103/ijo.IJO_904_17
Bilateral herpes simplex keratitis reactivation after lacrimal gland botulinum toxin injection
Abstract
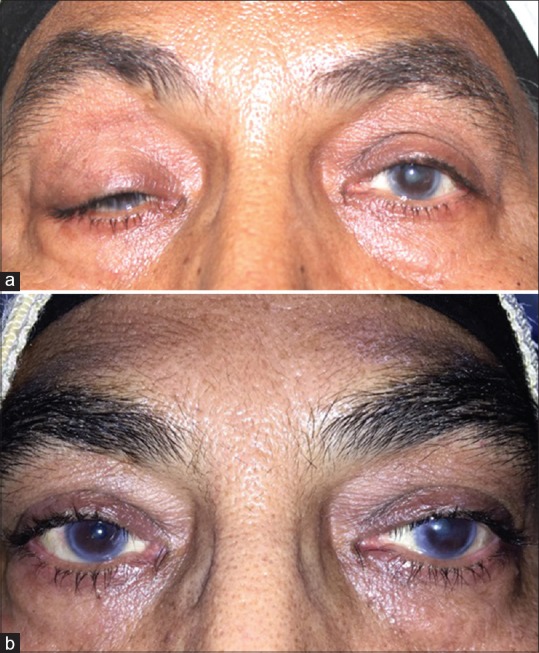
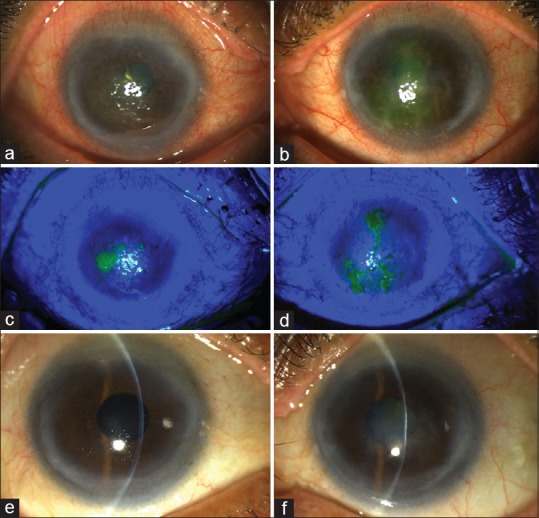
Botulinum toxin A (BTA) injections into lacrimal gland are being used for refractory epiphora due to intractable lacrimal disorders with success rates reported from 18% to 86%. Most common side effects are transient ptosis and diplopia. We report a case of a 59-year-old female injected with 2.5 units of BTA injection in each lacrimal gland for functional epiphora. The patient had a history of herpes simplex viral keratitis that was quiescent for more than 2 years. After 3 weeks, she developed reactivation of viral keratitis bilaterally, which was successfully managed with antivirals and topical steroids. Reactivation of quiescent herpes simplex keratitis is a possibility after lacrimal gland BTA and caution should be exercised in such cases.
Keywords: Botulinum toxin; functional epiphora; herpes simplex keratitis; lacrimal gland; reactivation.
Conflict of interest statement
There are no conflicts of interest
Figures
Similar articles
-
Reactivation of herpes simplex viral keratitis following the botulinum toxin injection.Indian J Ophthalmol. 2018 Feb;66(2):306-308. doi: 10.4103/ijo.IJO_714_17. Indian J Ophthalmol. 2018. PMID: 29380788 Free PMC article.
-
A review on use of botulinum toxin for intractable lacrimal drainage disorders.Int Ophthalmol. 2018 Oct;38(5):2233-2238. doi: 10.1007/s10792-017-0661-9. Epub 2017 Aug 1. Int Ophthalmol. 2018. PMID: 28766277 Review.
-
Modalities to decrease stromal herpes simplex keratitis reactivation rates.Arch Ophthalmol. 2010 Nov;128(11):1497; author reply 1497-8. doi: 10.1001/archophthalmol.2010.259. Arch Ophthalmol. 2010. PMID: 21060060 No abstract available.
-
Results of lacrimal gland botulinum toxin injection for epiphora in lacrimal obstruction and gustatory tearing.Ophthalmic Plast Reconstr Surg. 2011 Mar-Apr;27(2):119-21. doi: 10.1097/IOP.0b013e318201d1d3. Ophthalmic Plast Reconstr Surg. 2011. PMID: 21224749
-
Management of herpes simplex virus stromal keratitis: an evidence-based review.Surv Ophthalmol. 2009 Mar-Apr;54(2):226-34. doi: 10.1016/j.survophthal.2008.12.004. Surv Ophthalmol. 2009. PMID: 19298901 Review.
Cited by
-
Ocular manifestations of herpes simplex virus.Curr Opin Ophthalmol. 2019 Nov;30(6):525-531. doi: 10.1097/ICU.0000000000000618. Curr Opin Ophthalmol. 2019. PMID: 31567695 Free PMC article. Review.
-
Bilateral Multiple Herpetic Epithelial Keratitis: A Case Report and Review of the Literature.Cureus. 2024 May 25;16(5):e61079. doi: 10.7759/cureus.61079. eCollection 2024 May. Cureus. 2024. PMID: 38919237 Free PMC article.
-
Unusual herpetic reactivation in a young female following botox injection: a case report study.BMC Infect Dis. 2023 Oct 2;23(1):647. doi: 10.1186/s12879-023-08514-3. BMC Infect Dis. 2023. PMID: 37784014 Free PMC article.
-
Herpes simplex keratitis: A brief clinical overview.World J Virol. 2024 Mar 25;13(1):89934. doi: 10.5501/wjv.v13.i1.89934. World J Virol. 2024. PMID: 38616855 Free PMC article. Review.
-
Incidence and Risk Factors of Bilateral Herpetic Keratitis: 2022 Update.Trop Med Infect Dis. 2022 Jun 7;7(6):92. doi: 10.3390/tropicalmed7060092. Trop Med Infect Dis. 2022. PMID: 35736971 Free PMC article. Review.
References
-
- Singh S, Ali MJ, Paulsen F. A review on use of botulinum toxin for intractable lacrimal drainage disorders. EyInt Ophthalmol. 2017 [Epub ahead of print] - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
