

Implications of current therapeutic restrictions for primaquine and tafenoquine in the radical cure of vivax malaria
- PMID: 29677199
- PMCID: PMC5931686
- DOI: 10.1371/journal.pntd.0006440
Implications of current therapeutic restrictions for primaquine and tafenoquine in the radical cure of vivax malaria
Abstract
Background: The 8-aminoquinoline antimalarials, the only drugs which prevent relapse of vivax and ovale malaria (radical cure), cause dose-dependent oxidant haemolysis in individuals with glucose-6-phosphate dehydrogenase (G6PD) deficiency. Patients with <30% and <70% of normal G6PD activity are not given standard regimens of primaquine and tafenoquine, respectively. Both drugs are currently considered contraindicated in pregnant and lactating women.
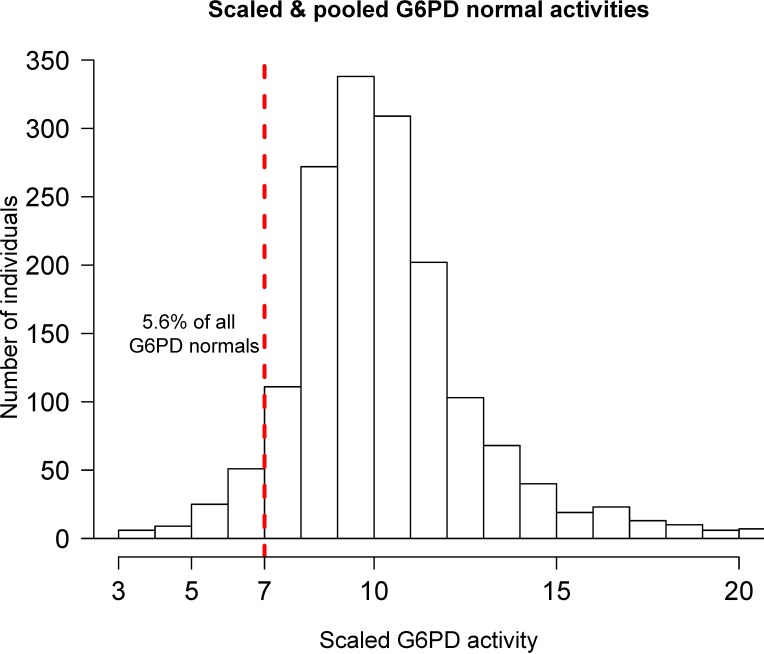
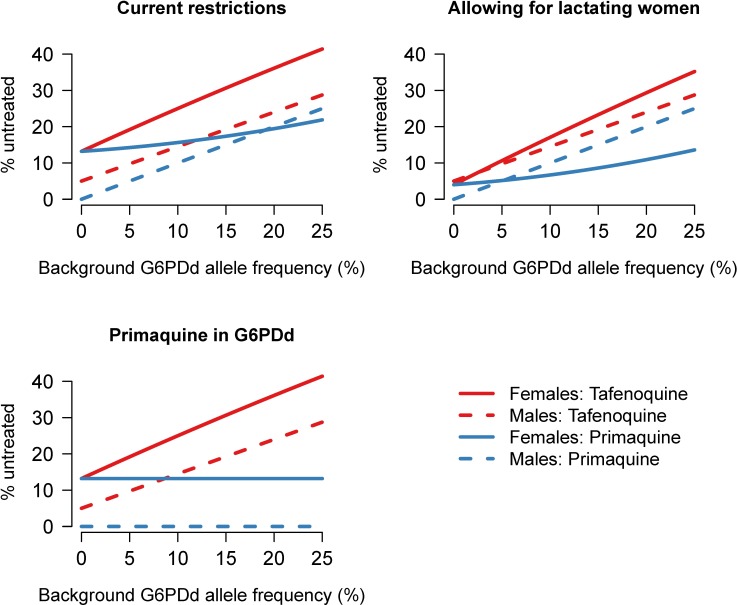
Methods: Quantitative G6PD enzyme activity data from 5198 individuals were used to estimate the proportions of heterozygous females who would be ineligible for treatment at the 30% and 70% activity thresholds, and the relationship with the severity of the deficiency. This was used to construct a simple model relating allele frequency in males to the potential population coverage of tafenoquine and primaquine under current prescribing restrictions.
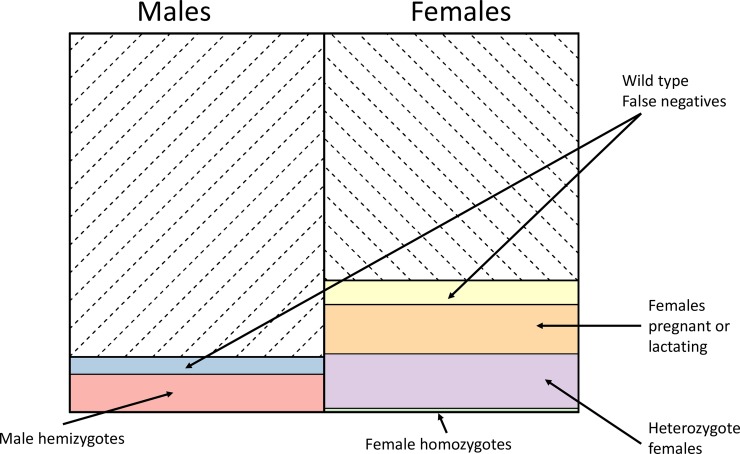
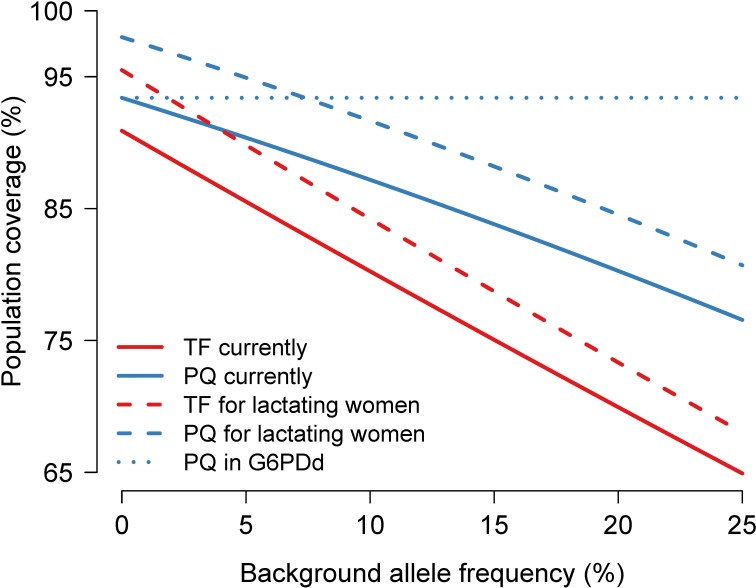
Findings: Independent of G6PD deficiency, the current pregnancy and lactation restrictions will exclude ~13% of females from radical cure treatment. This could be reduced to ~4% if 8-aminoquinolines can be prescribed to women breast-feeding infants older than 1 month. At a 30% activity threshold, approximately 8-19% of G6PD heterozygous women are ineligible for primaquine treatment; at a 70% threshold, 50-70% of heterozygous women and approximately 5% of G6PD wild type individuals are ineligible for tafenoquine treatment. Thus, overall in areas where the G6PDd allele frequency is >10% more than 15% of men and more than 25% of women would be unable to receive tafenoquine. In vivax malaria infected patients these proportions will be lowered by any protective effect against P. vivax conferred by G6PD deficiency.
Conclusion: If tafenoquine is deployed for radical cure, primaquine will still be needed to obtain high population coverage. Better radical cure antimalarial regimens are needed.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Howes RE, Battle KE, Mendis KN, Smith DL, Cibulskis RE, Baird JK, et al. Global Epidemiology of Plasmodium vivax. Am J Trop Med Hyg. The American Society of Tropical Medicine and Hygiene; 2016;95: 15–34. doi: 10.4269/ajtmh.16-0141 - DOI - PMC - PubMed
-
- Betuela I, Rosanas-Urgell A, Kiniboro B, Stanisic DI, Samol L, de Lazzari E, et al. Relapses Contribute Significantly to the Risk of Plasmodium vivax Infection and Disease in Papua New Guinean Children 1–5 Years of Age. J Infect Dis. 2012;206: 1771–1780. doi: 10.1093/infdis/jis580 - DOI - PubMed
-
- White NJ. Determinants of relapse periodicity in Plasmodium vivax malaria. Malar J. BioMed Central; 2011;10: 297 doi: 10.1186/1475-2875-10-297 - DOI - PMC - PubMed
-
- John GK, Douglas NM, von Seidlein L, Nosten F, Baird J, White NJ, et al. Primaquine radical cure of Plasmodium vivax: a critical review of the literature. Malar J. BioMed Central; 2012;11: 280 doi: 10.1186/1475-2875-11-280 - DOI - PMC - PubMed
-
- Leslie T, Rab MA, Ahmadzai H, Durrani N, Fayaz M, Kolaczinski J, et al. Compliance with 14-day primaquine therapy for radical cure of vivax malaria—a randomized placebo-controlled trial comparing unsupervised with supervised treatment. Trans R Soc Trop Med Hyg. 2004;98: 168–73. Available: http://www.ncbi.nlm.nih.gov/pubmed/15024927 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
