

Effect of Uterosacral Ligament Suspension vs Sacrospinous Ligament Fixation With or Without Perioperative Behavioral Therapy for Pelvic Organ Vaginal Prolapse on Surgical Outcomes and Prolapse Symptoms at 5 Years in the OPTIMAL Randomized Clinical Trial
- PMID: 29677302
- PMCID: PMC5933329
- DOI: 10.1001/jama.2018.2827
Effect of Uterosacral Ligament Suspension vs Sacrospinous Ligament Fixation With or Without Perioperative Behavioral Therapy for Pelvic Organ Vaginal Prolapse on Surgical Outcomes and Prolapse Symptoms at 5 Years in the OPTIMAL Randomized Clinical Trial
Abstract
Importance: Uterosacral ligament suspension (ULS) and sacrospinous ligament fixation (SSLF) are commonly performed pelvic organ prolapse procedures despite a lack of long-term efficacy data.
Objective: To compare outcomes in women randomized to (1) ULS or SSLF and (2) usual care or perioperative behavioral therapy and pelvic floor muscle training (BPMT) for vaginal apical prolapse.
Design, setting, and participants: This 2 × 2 factorial randomized clinical trial was conducted at 9 US medical centers. Eligible participants who completed the Operations and Pelvic Muscle Training in the Management of Apical Support Loss Trial enrolled between January 2008 and March 2011 and were followed up 5 years after their index surgery from April 2011 through June 2016.
Interventions: Two randomizations: (1) BPMT (n = 186) or usual care (n = 188) and (2) surgical intervention (ULS: n = 188 or SSLF: n = 186).
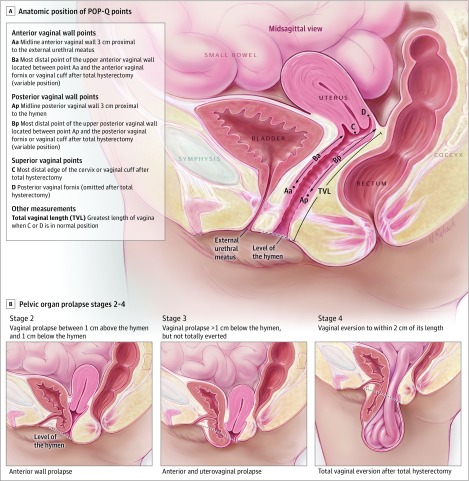
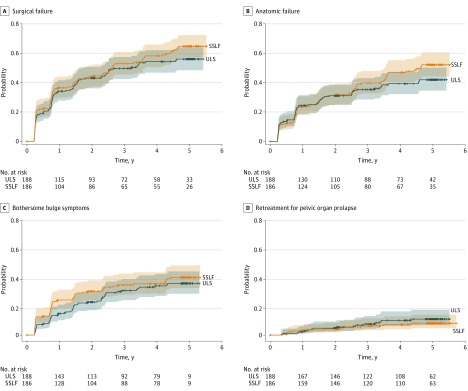
Main outcomes and measures: The primary surgical outcome was time to surgical failure. Surgical failure was defined as (1) apical descent greater than one-third of total vaginal length or anterior or posterior vaginal wall beyond the hymen or retreatment for prolapse (anatomic failure), or (2) bothersome bulge symptoms. The primary behavioral outcomes were time to anatomic failure and Pelvic Organ Prolapse Distress Inventory scores (range, 0-300).
Results: The original study randomized 374 patients, of whom 309 were eligible for this extended trial. For this study, 285 enrolled (mean age, 57.2 years), of whom 244 (86%) completed the extended trial. By year 5, the estimated surgical failure rate was 61.5% in the ULS group and 70.3% in the SSLF group (adjusted difference, -8.8% [95% CI, -24.2 to 6.6]). The estimated anatomic failure rate was 45.6% in the BPMT group and 47.2% in the usual care group (adjusted difference, -1.6% [95% CI, -21.2 to 17.9]). Improvements in Pelvic Organ Prolapse Distress Inventory scores were -59.4 in the BPMT group and -61.8 in the usual care group (adjusted mean difference, 2.4 [95% CI, -13.7 to 18.4]).
Conclusions and relevance: Among women who had undergone vaginal surgery for apical pelvic organ vaginal prolapse, there was no significant difference between ULS and SSLF in rates of surgical failure and no significant difference between perioperative behavioral muscle training and usual care on rates of anatomic success and symptom scores at 5 years. Compared with outcomes at 2 years, rates of surgical failure increased during the follow-up period, although prolapse symptom scores remained improved.
Trial registration: clinicaltrials.gov Identifier: NCT01166373.
Conflict of interest statement
Figures

Comment in
-
Re: Effect of Uterosacral Ligament Suspension vs Sacrospinous Ligament Fixation with or without Perioperative Behavioral Therapy for Pelvic Organ Vaginal Prolapse on Surgical Outcomes and Prolapse Symptoms at 5 Years in the OPTIMAL Randomized Clinical Trial.J Urol. 2018 Oct;200(4):704-705. doi: 10.1016/j.juro.2018.07.033. Epub 2018 Jul 17. J Urol. 2018. PMID: 30227590 No abstract available.
References
-
- Jelovsek JE, Maher C, Barber MD. Pelvic organ prolapse. Lancet. 2007;369(9566):1027-1038. - PubMed
-
- Committee on Practice Bulletins-Gynecology, American Urogynecologic Society Practice bulletin No. 185: pelvic organ prolapse. Obstet Gynecol. 2017;130(5):e234-e250. - PubMed
-
- Diwadkar GB, Barber MD, Feiner B, Maher C, Jelovsek JE. Complication and reoperation rates after apical vaginal prolapse surgical repair: a systematic review. Obstet Gynecol. 2009;113(2 pt 1):367-373. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
