

The increasing burden and complexity of multi-morbidity and polypharmacy in geriatric HIV patients: a cross sectional study of people aged 65 - 74 years and more than 75 years
- PMID: 29678160
- PMCID: PMC5910563
- DOI: 10.1186/s12877-018-0789-0
The increasing burden and complexity of multi-morbidity and polypharmacy in geriatric HIV patients: a cross sectional study of people aged 65 - 74 years and more than 75 years
Abstract
Background: Geriatric Patients Living with HIV/AIDS (GEPPO) is a new prospective observational multicentre cohort consisting of all the HIV-positive geriatric patients being treated at 10 clinics in Italy, and HIV-negative controls attending a single geriatric clinic. The aim of this analysis of the GEPPO cohort was to compare prevalence and risk factors of individual non-communicable diseases (NCD), multi-morbidity (MM) and polypharmacy (PP) amongst HIV positive and HIV negative controls at enrolment into the GEPPO cohort.
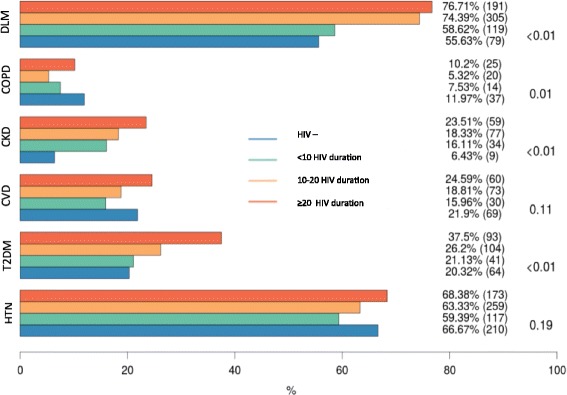
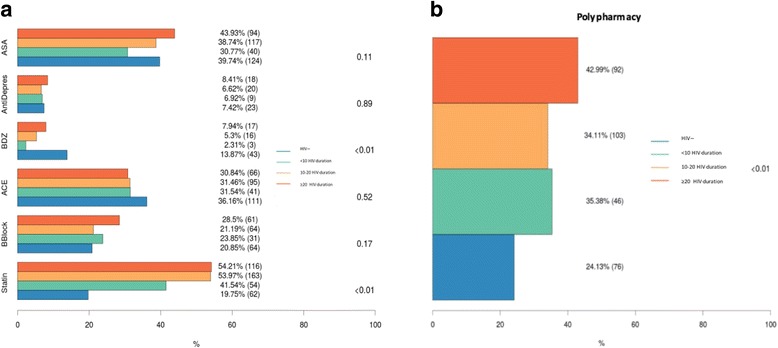
Methods: This cross-sectional study was conducted between June 2015 and May 2016. The duration of HIV infection was subdivided into three intervals: < 10, 10-20 and > 20 years. The NCD diagnoses were based on guidelines defined criteria, including cardiovascular disease, hypertension, type 2 diabetes, chronic kidney disease, dyslipidaemia, chronic obstructive pulmonary disease. MM was classified as the presence of two or more co-morbidities. The medications prescribed for the treatment of comorbidities were collected in both HIV positive and HIV negative group from patient files and were categorized using the Anatomical Therapeutic Chemical (ATC) classification. PP was defined as the presence of five or more drug components other than anti-retroviral agents.
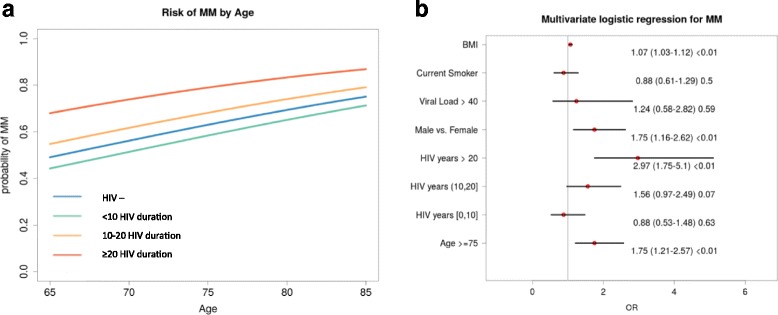
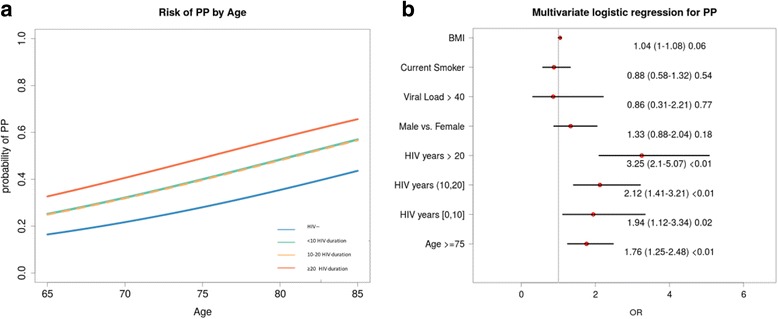
Results: The study involved a total of 1573 patient: 1258 HIV positive and 315 HIV negative). The prevalence of individual comorbidities was similar in the two groups with the exception of dyslipidaemia, which was more frequent in the HIV-positive patients (p < 0.01). When the HIV-positive group was stratified based on the duration of HIV infection, most of the co-morbidities were significantly more frequent than in control patients, except for hypertension and cardiovascular disease, while COPD was more prevalent in the control group. MM and PP were both more prevalent in the HIV-positive group, respectively 64% and 37%.
Conclusions: MM and PP burden in geriatric HIV positive patients are related to longer duration of HIV-infection rather than older age per se.
Keywords: Geriatric HIV-infected population; Multi-morbidity; Polypharmacy.
Conflict of interest statement
Authors’ information
Giovanni Guaraldi, MD, is Associate Professor of Infectious disease at the University of Modena and Reggio Emilia. Since the year 2000, he has lead the Modena HIV Metabolic Clinic (MHMC). This referral centre offers a multidisciplinary team approach to HIV patients with metabolic abnormalities, and it offers a multidimensional evaluation of ageing HIV infected patients. More than 4500 patients are followed at this Centre.
Prof. Guaraldi published over 300 peer reviewed papers mainly focused on frailty and HIV associated co-morbidities.
In 2016 he built the first HIV geriatric cohort in Italy called: Geriatric Patients Living with HIV/AIDS (GEPPO).
Two peer reviewed papers have been published.
about this new prospective observational multicentre cohort:
Calcagno A, Piconi S, Focà E, Nozza S, Carli F, Montrucchio C, Cattelan AM, Orofino G, Celesia BM, Morena V, De Socio GV, Guaraldi G;
GEPPO (GEriatric Patients living with HIV/AIDS: a Prospective Multidimensional cOhort) Study Group. Role of Normalized T-Cell Subsets in Predicting Comorbidities in a Large Cohort of Geriatric HIV-infected Patient. J Acquir Immune Defic Syndr. 2017 Jul 8. doi: 10.1097/QAI.0000000000001496. [Epub ahead of print]Nozza S, Malagoli A, Maia L, Calcagno A, Focà E, De Socio G, Piconi S, Orofino G, Cattelan AM, Celesia BM, Gervasi E, Guaraldi G;
GEPPO Study Group. Antiretroviral therapy in geriatric HIV patients: the GEPPO cohort study. J Antimicrob Chemother. 2017 Jun 10. doi: 10.1093/jac/dkx169. [Epub ahead of print] PMID:28605493
Ethics approval and consent to participate
The study received approval from Comitato Etico Provinciale di Modena.
Study 39/2016. IRB approval: Prot.1710 of 10 May 2016.
Written informed consent was obtained from participants.
Consent for publication
The paper contains aggregated data only.
Competing interests
GG received research grants from ViiV Healthcare, Gilead, Merck Sharp and Dohme (MSD). Talks grants from ViiV Healthcare, Gilead, Merck Sharp and Dohme, Jansen, BMS. Consultation to ViiV Healthcare, Gilead, Merck Sharp and Dohme. CA received grants, travel grants and speaker’s honoraria from Abbvie, BMS, Gilead, ViiV Healthcare, Janssen-Cilag and MSD. CBM received grants, travel grants and speaker’s honoraria from Abbvie, BMS, Gilead, ViiV Healthcare, Janssen-Cilag and MSD. DSGV received travel grants from Abbvie, BMS, Gilead, ViiV Healthcare, Janssen-Cilag and MSD. CAM received grants and speaker’s honoraria from Abbvie, BMS, Gilead, ViiV Healthcare, Janssen-Cilag and MSD. NS received travel grants and speaker’s honoraria from Abbvie, BMS, Gilead, ViiV Healthcare, Janssen-Cilag and MSD. OG received travel grants and speaker’s honoraria from Abbvie, BMS, Gilead, ViiV Healthcare, Janssen-Cilag and MSD. RA grants, travel grants and speaker’s honoraria from BMS, Gilead, ViiV Healthcare, Janssen-Cilag, Novartis and MSD. FE received travel grants and speaker’s honoraria from BMS, Gilead, ViiV Healthcare, Janssen-Cilag and MSD. DPG received grants, travel grants and speaker’s honoraria from Abbvie, BMS, Gilead, ViiV Healthcare, Janssen-Cilag and MSD. MA, MC, CF, PS reported no potential conflict of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
