

Stress Myocardial Blood Flow Heterogeneity Is a Positron Emission Tomography Biomarker of Ventricular Arrhythmias in Patients With Hypertrophic Cardiomyopathy
- PMID: 29678336
- PMCID: PMC5966031
- DOI: 10.1016/j.amjcard.2018.01.022
Stress Myocardial Blood Flow Heterogeneity Is a Positron Emission Tomography Biomarker of Ventricular Arrhythmias in Patients With Hypertrophic Cardiomyopathy
Abstract
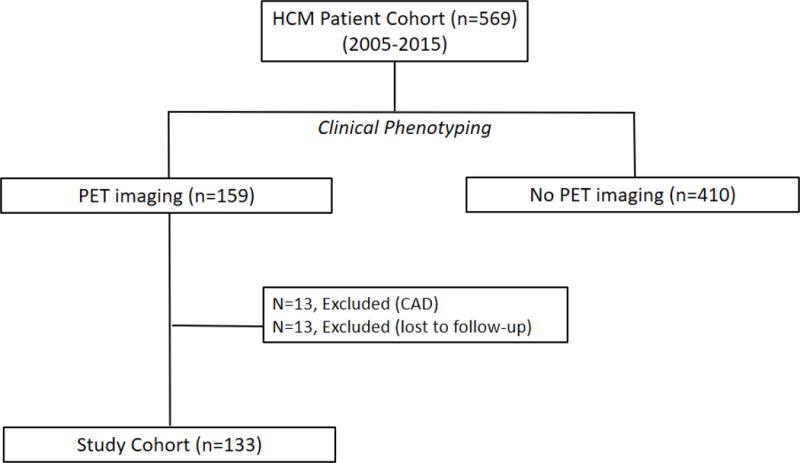
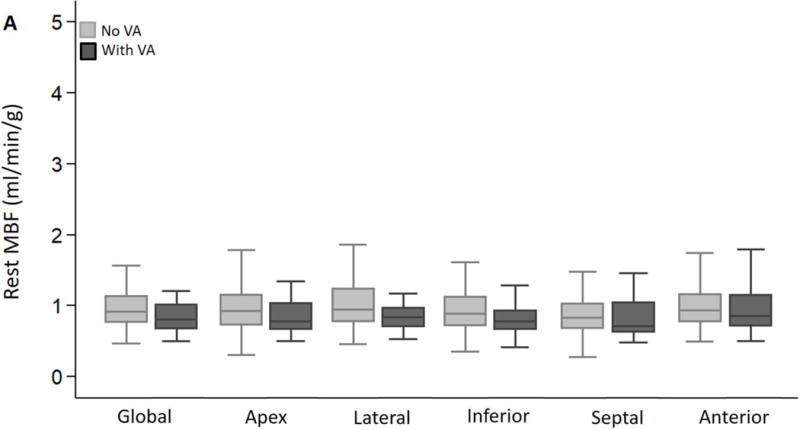
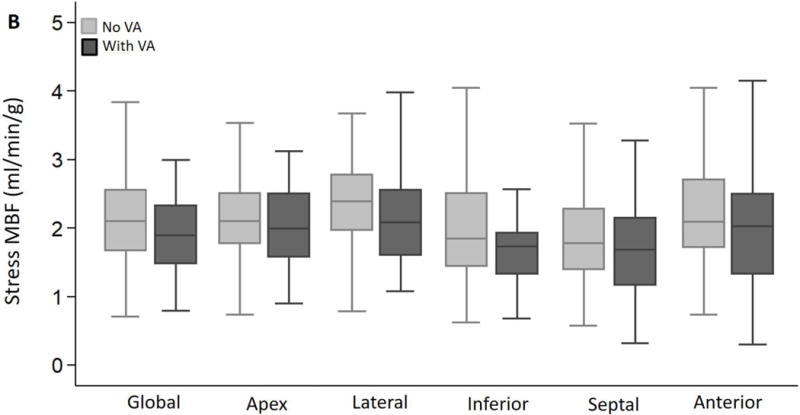
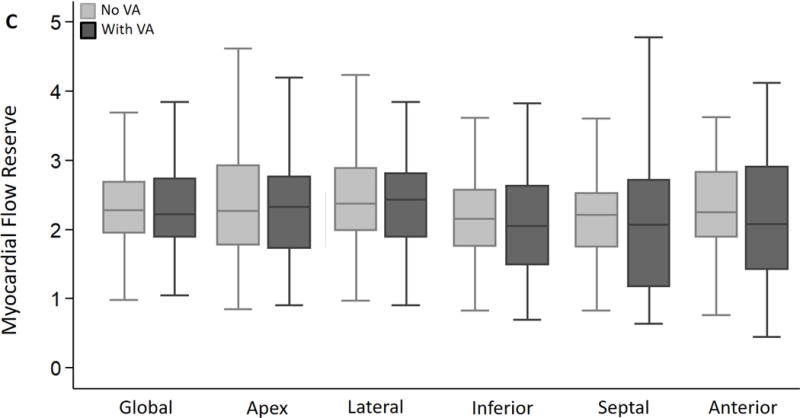
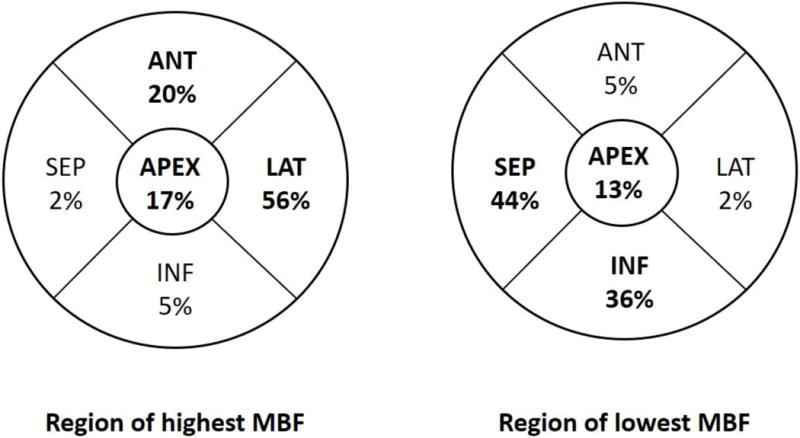
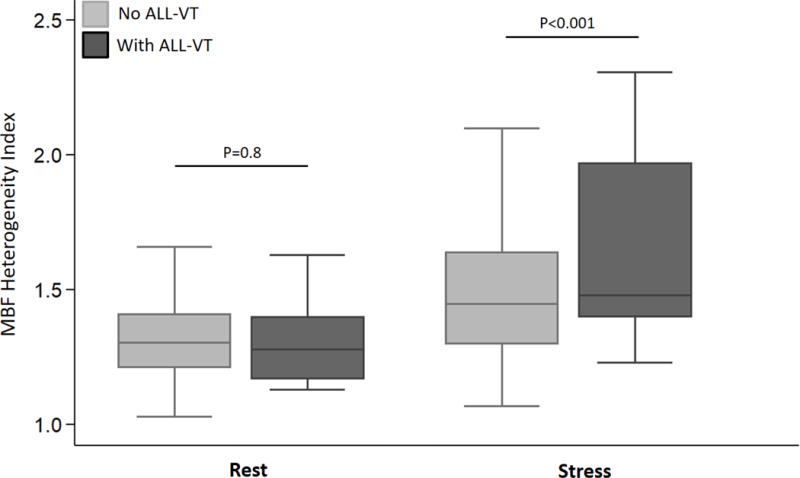
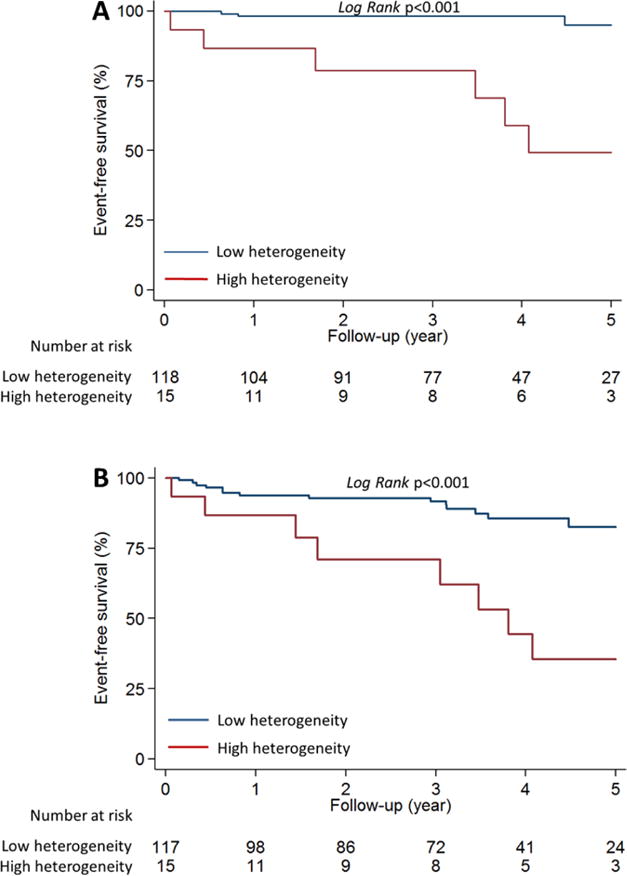
Patients with hypertrophic cardiomyopathy (HC) are at increased risk of sudden cardiac death. Abnormalities in myocardial blood flow (MBF) detected by positron emission tomography (PET) are common in HC, but a PET marker that identifies patients at risk of sudden cardiac death is lacking. We hypothesized that disparities in regional myocardial perfusion detected by PET would identify patients with HC at risk of ventricular arrhythmias. To test this hypothesis, we quantified global and regional MBFs by 13NH3-PET at rest and at stress, and developed a heterogeneity index to assess MBF heterogeneity in 133 symptomatic patients with HC. The MBF heterogeneity index was computed by dividing the highest by the lowest regional MBF value, at rest and after vasodilator stress, in each patient. High stress MBF heterogeneity was defined as an index of ≧1.85. Patients with HC were stratified by the presence or the absence of ventricular arrhythmias, defined as sustained ventricular tachycardia (VT) and/or nonsustained VT, during follow-up. We found that global and regional MBFs at rest and stress were similar in patients with HC with or without ventricular arrhythmias. Variability in regional stress MBF was observed in both groups, but the stress MBF heterogeneity index was significantly higher in patients with HC who developed ventricular arrhythmias (1.82 ± 0.77 vs 1.49 ± 0.25, p <0.001). A stress MBF heterogeneity index of ≧1.85 was an independent predictor of both sustained VT (hazard ratio 16.1, 95% confidence interval 3.2 to 80.3) and all-VT (sustained-VT + nonsustained VT: hazard ratio 3.7, 95% confidence interval 1.4 to 9.7). High heterogeneity of stress MBF, reflected by an MBF heterogeneity index of ≥1.85, is a PET biomarker for ventricular arrhythmias in symptomatic patients with HC.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest: None
Figures
References
-
- Gersh BJ, Maron BJ, Bonow RO, Dearani JA, Fifer MA, Link MS, Naidu SS, Nishimura RA, Ommen SR, Rakowski H, Seidman CE, Towbin JA, Udelson JE, Yancy CW, American College of Cardiology Foundation/American Heart Association Task Force on Practice G 2011 ACCF/AHA Guideline for the Diagnosis and Treatment of Hypertrophic Cardiomyopathy: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Developed in collaboration with the American Association for Thoracic Surgery, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;58:e212–260. - PubMed
-
- Jung WI, Sieverding L, Breuer J, Hoess T, Widmaier S, Schmidt O, Bunse M, van Erckelens F, Apitz J, Lutz O, Dietze GJ. 31P NMR spectroscopy detects metabolic abnormalities in asymptomatic patients with hypertrophic cardiomyopathy. Circulation. 1998;97:2536–2542. - PubMed
-
- Dass S, Cochlin LE, Suttie JJ, Holloway CJ, Rider OJ, Carden L, Tyler DJ, Karamitsos TD, Clarke K, Neubauer S, Watkins H. Exacerbation of cardiac energetic impairment during exercise in hypertrophic cardiomyopathy: a potential mechanism for diastolic dysfunction. Eur Heart J. 2015;36:1547–1554. - PubMed
-
- Cecchi F, Olivotto I, Gistri R, Lorenzoni R, Chiriatti G, Camici PG. Coronary microvascular dysfunction and prognosis in hypertrophic cardiomyopathy. N Engl J Med. 2003;349:1027–1035. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
