

Gaps in Guidelines for the Management of Diabetes in Low- and Middle-Income Versus High-Income Countries-A Systematic Review
- PMID: 29678866
- PMCID: PMC5911785
- DOI: 10.2337/dc17-1795
Gaps in Guidelines for the Management of Diabetes in Low- and Middle-Income Versus High-Income Countries-A Systematic Review
Abstract
Objective: The extent to which diabetes (DM) practice guidelines, often based on evidence from high-income countries (HIC), can be implemented to improve outcomes in low- and middle-income countries (LMIC) is a critical challenge. We carried out a systematic review to compare type 2 DM guidelines in individual LMIC versus HIC over the past decade to identify aspects that could be improved to facilitate implementation.
Research design and methods: Eligible guidelines were sought from online databases and websites of diabetes associations and ministries of health. Type 2 DM guidelines published between 2006 and 2016 with accessible full publications were included. Each of the 54 eligible guidelines was assessed for compliance with the Institute of Medicine (IOM) standards, coverage of the cardiovascular quadrangle (epidemiologic surveillance, prevention, acute care, and rehabilitation), translatability, and its target audiences.
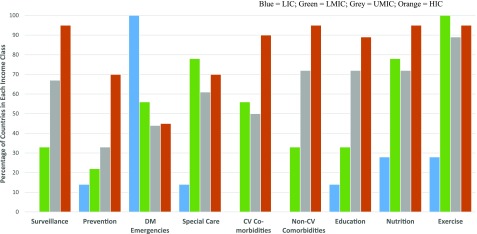
Results: Most LMIC guidelines were inadequate in terms of applicability, clarity, and dissemination plan as well as socioeconomic and ethical-legal contextualization. LMIC guidelines targeted mainly health care providers, with only a few including patients (7%), payers (11%), and policy makers (18%) as their target audiences. Compared with HIC guidelines, the spectrum of DM clinical care addressed by LMIC guidelines was narrow. Most guidelines from the LMIC complied with less than half of the IOM standards, with 12% of the LMIC guidelines satisfying at least four IOM criteria as opposed to 60% of the HIC guidelines (P < 0.001).
Conclusions: A new approach to the contextualization, content development, and delivery of LMIC guidelines is needed to improve outcomes.
© 2018 by the American Diabetes Association.
Figures



References
-
- World Health Organization. Global Report on Diabetes. Geneva, World Health Organization, 2016
-
- Yusuf S, Rangarajan S, Teo K, et al. ; PURE Investigators . Cardiovascular risk and events in 17 low-, middle-, and high-income countries. N Engl J Med 2014;371:818–827 - PubMed
-
- Minton EA, Kahle LR. Belief Systems, Religion, and Behavioral Economics: Marketing in Multicultural Environments. New York, Business Expert Press, 2014
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
