

Autoantibodies and scleroderma phenotype define subgroups at high-risk and low-risk for cancer
- PMID: 29678941
- PMCID: PMC6272061
- DOI: 10.1136/annrheumdis-2018-212999
Autoantibodies and scleroderma phenotype define subgroups at high-risk and low-risk for cancer
Abstract
Objectives: Recent studies demonstrate autoantibodies are powerful tools to interrogate molecular events linking cancer and the development of autoimmunity in scleroderma. Investigating cancer risk in these biologically relevant subsets may provide an opportunity to develop personalised cancer screening guidelines. In this study, we examined cancer risk in distinct serologic and phenotypic scleroderma subsets and compared estimates with the general population.
Methods: Patients in the Johns Hopkins Scleroderma Center observational cohort were studied. Overall and site-specific cancer incidence was calculated in distinct autoantibody and scleroderma phenotypic subsets, and compared with the Surveillance, Epidemiology and End Results registry, a representative sample of the US population.
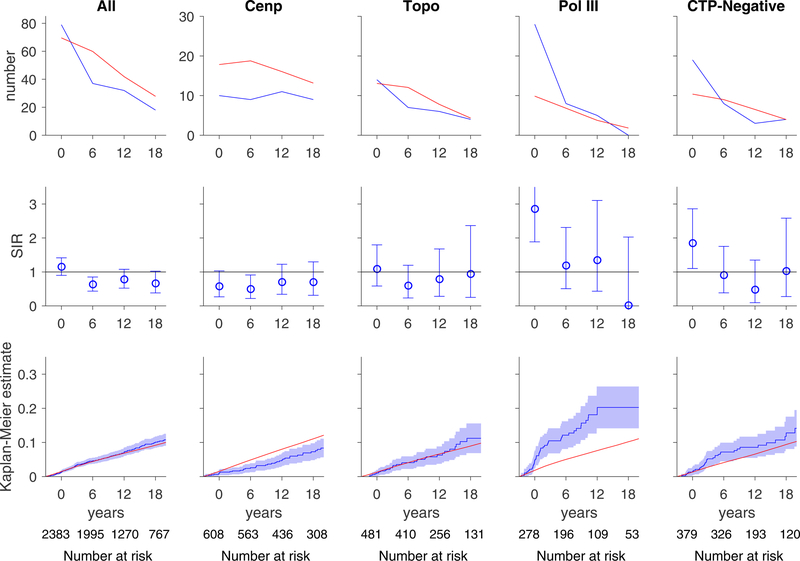
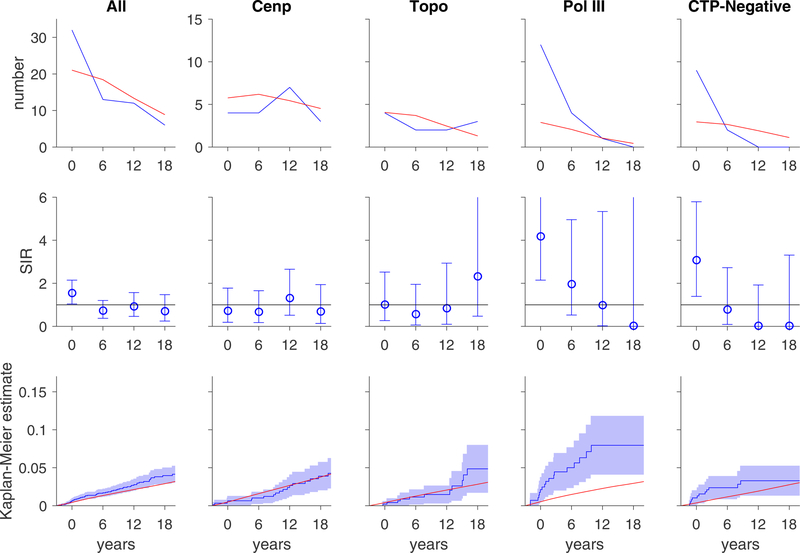
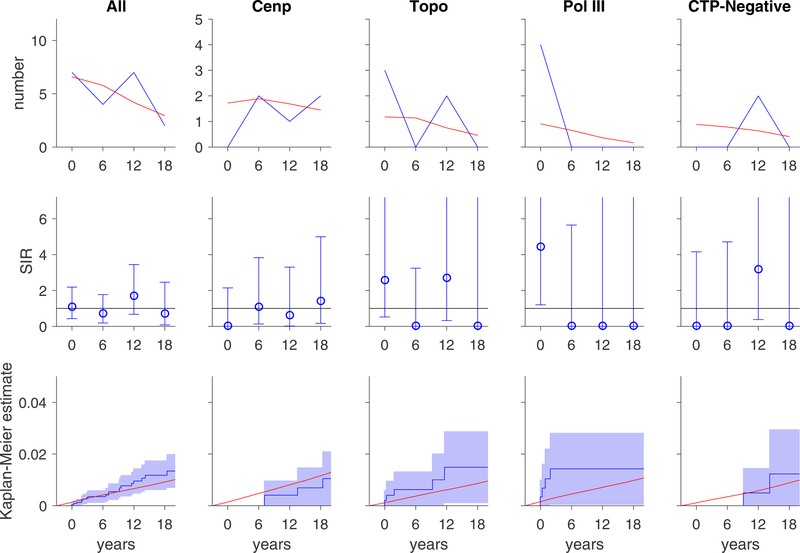
Results: 2383 patients with scleroderma contributing 37 686 person-years were studied. 205 patients (8.6%) had a diagnosis of cancer. Within 3 years of scleroderma onset, cancer risk was increased in patients with RNA polymerase III autoantibodies (antipol; standardised incidence ratio (SIR) 2.84, 95% CI 1.89 to 4.10) and those lacking centromere, topoisomerase-1 and pol antibodies (SIR 1.83, 95% CI 1.10 to 2.86). Among antipol-positive patients, cancer-specific risk may vary by scleroderma subtype; those with diffuse scleroderma had an increased breast cancer risk, whereas those with limited scleroderma had high lung cancer risk. In contrast, patients with anticentromere antibodies had a lower risk of cancer during follow-up (SIR 0.59, 95% CI 0.44 to 0.76).
Conclusions: Autoantibody specificity and disease subtype are biologically meaningful filters that may inform cancer risk stratification in patients with scleroderma. Future research testing the value of targeted cancer screening strategies in patients with scleroderma is needed.
Keywords: autoantibodies; epidemiology; systemic sclerosis.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: TI, LC-R, AR and AAS have recently submitted a patent application entitled ’Materials and Methods for Assessing Cancer Risk and Treating Cancer'.
Figures
References
-
- Abu-Shakra M, Guillemin F, Lee P. Cancer in systemic sclerosis. Arthritis rheum 1993;36(4):460–4. [published Online First: 1993/04/01] - PubMed
-
- Derk CT, Rasheed M, Artlett CM, et al. A cohort study of cancer incidence in systemic sclerosis. J Rheumatol 2006;33(6):1113–6. [published Online First: 2006/04/20] - PubMed
-
- Kang KY, Yim HW, Kim IJ, et al. Incidence of cancer among patients with systemic sclerosis in Korea: results from a single centre. Scand J Rheumatol 2009;38(4):299–303. doi: 10.1080/03009740802642062 - DOI - PubMed
-
- Kuo CF, Luo SF, Yu KH, et al. Cancer risk among patients with systemic sclerosis: a nationwide population study in Taiwan. Scand J Rheumatol 2012;41(1):44–9. doi: 10.3109/03009742.2011.618145 [published Online First: 2011/12/14] - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
