

Middle East respiratory syndrome coronavirus: risk factors and determinants of primary, household, and nosocomial transmission
- PMID: 29680581
- PMCID: PMC7164784
- DOI: 10.1016/S1473-3099(18)30127-0
Middle East respiratory syndrome coronavirus: risk factors and determinants of primary, household, and nosocomial transmission
Abstract
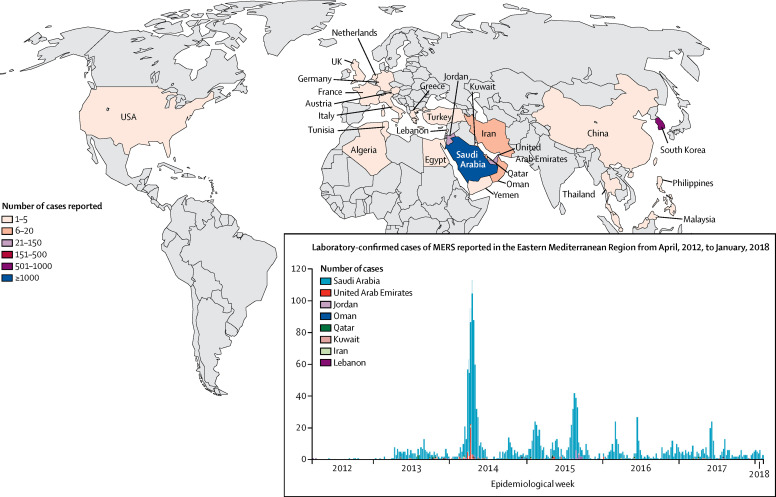
Middle East respiratory syndrome coronavirus (MERS-CoV) is a lethal zoonosis that causes death in 35·7% of cases. As of Feb 28, 2018, 2182 cases of MERS-CoV infection (with 779 deaths) in 27 countries were reported to WHO worldwide, with most being reported in Saudi Arabia (1807 cases with 705 deaths). MERS-CoV features prominently in the WHO blueprint list of priority pathogens that threaten global health security. Although primary transmission of MERS-CoV to human beings is linked to exposure to dromedary camels (Camelus dromedarius), the exact mode by which MERS-CoV infection is acquired remains undefined. Up to 50% of MERS-CoV cases in Saudi Arabia have been classified as secondary, occurring from human-to-human transmission through contact with asymptomatic or symptomatic individuals infected with MERS-CoV. Hospital outbreaks of MERS-CoV are a hallmark of MERS-CoV infection. The clinical features associated with MERS-CoV infection are not MERS-specific and are similar to other respiratory tract infections. Thus, the diagnosis of MERS can easily be missed, unless the doctor or health-care worker has a high degree of clinical awareness and the patient undergoes specific testing for MERS-CoV. The largest outbreak of MERS-CoV outside the Arabian Peninsula occurred in South Korea in May, 2015, resulting in 186 cases with 38 deaths. This outbreak was caused by a traveller with undiagnosed MERS-CoV infection who became ill after returning to Seoul from a trip to the Middle East. The traveller visited several health facilities in South Korea, transmitting the virus to many other individuals long before a diagnosis was made. With 10 million pilgrims visiting Saudi Arabia each year from 182 countries, watchful surveillance by public health systems, and a high degree of clinical awareness of the possibility of MERS-CoV infection is essential. In this Review, we provide a comprehensive update and synthesis of the latest available data on the epidemiology, determinants, and risk factors of primary, household, and nosocomial transmission of MERS-CoV, and suggest measures to reduce risk of transmission.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Controversies regarding shielding and susceptibility to COVID-19 disease in liver transplant recipients in the United Kingdom.Transpl Infect Dis. 2020 Oct;22(5):e13352. doi: 10.1111/tid.13352. Epub 2020 Jun 17. Transpl Infect Dis. 2020. PMID: 32500939 Free PMC article. No abstract available.
References
-
- Peiris JS, Yuen KY, Osterhaus AD, Stöhr K. The severe acute respiratory syndrome. N Engl J Med. 2003;349:2431–2441. - PubMed
-
- WHO Severe acute respiratory syndrome. http://www.who.int/topics/sars/en/ (accessed March 28, 2018).
-
- Hui DS, Memish ZA, Zumla A. Severe acute respiratory syndrome vs the Middle East respiratory syndrome. Curr Opin Pulm Med. 2014;20:233–241. - PubMed
-
- WHO Middle East respiratory syndrome coronavirus (MERS-CoV) http://www.who.int/emergencies/mers-cov/en/ (accessed Jan 16, 2018).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
