

Home treatment of COPD exacerbation selected by DECAF score: a non-inferiority, randomised controlled trial and economic evaluation
- PMID: 29680821
- PMCID: PMC6204956
- DOI: 10.1136/thoraxjnl-2017-211197
Home treatment of COPD exacerbation selected by DECAF score: a non-inferiority, randomised controlled trial and economic evaluation
Abstract
Background: Previous models of Hospital at Home (HAH) for COPD exacerbation (ECOPD) were limited by the lack of a reliable prognostic score to guide patient selection. Approximately 50% of hospitalised patients have a low mortality risk by DECAF, thus are potentially suitable.
Methods: In a non-inferiority randomised controlled trial, 118 patients admitted with a low-risk ECOPD (DECAF 0 or 1) were recruited to HAH or usual care (UC). The primary outcome was health and social costs at 90 days.
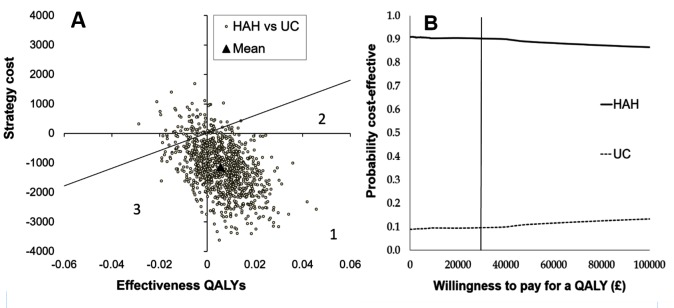
Results: Mean 90-day costs were £1016 lower in HAH, but the one-sided 95% CI crossed the non-inferiority limit of £150 (CI -2343 to 312). Savings were primarily due to reduced hospital bed days: HAH=1 (IQR 1-7), UC=5 (IQR 2-12) (P=0.001). Length of stay during the index admission in UC was only 3 days, which was 2 days shorter than expected. Based on quality-adjusted life years, the probability of HAH being cost-effective was 90%. There was one death within 90 days in each arm, readmission rates were similar and 90% of patients preferred HAH for subsequent ECOPD.
Conclusion: HAH selected by low-risk DECAF score was safe, clinically effective, cost-effective, and preferred by most patients. Compared with earlier models, selection is simpler and approximately twice as many patients are eligible. The introduction of DECAF was associated with a fall in UC length of stay without adverse outcome, supporting use of DECAF to direct early discharge.
Trial registration number: Registered prospectively ISRCTN29082260.
Keywords: copd exacerbations.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: SCB reports grants from NIHR: Research for Patient Benefit Programme, during the conduct of the study; HTA funding, grants from Philips Respironics and Pfizer Open Air, personal fees from Pfizer and AstraZeneca, outside the submitted work. JG reports grants from NIHR Research for Patient Benefit, during the conduct of the study. CE, GJG, TH, AJS and JS have no competing interests to declare.
Figures


Comment in
-
People with chronic obstructive pulmonary disease exacerbations prefer early discharge, then treatment at home.BMJ. 2019 Feb 19;364:k5339. doi: 10.1136/bmj.k5339. BMJ. 2019. PMID: 30782586
References
-
- National Clinical Guideline Centre. Chronic obstructive pulmonary disease: management of chronic obstructive pulmonary disease in adults in primary and secondary care. London: National Clinical Guideline Centre, 2010. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical