

Ultrasonic Cavitation-Enabled Treatment for Therapy of Hypertrophic Cardiomyopathy: Proof of Principle
- PMID: 29681423
- PMCID: PMC5960614
- DOI: 10.1016/j.ultrasmedbio.2018.03.010
Ultrasonic Cavitation-Enabled Treatment for Therapy of Hypertrophic Cardiomyopathy: Proof of Principle
Abstract
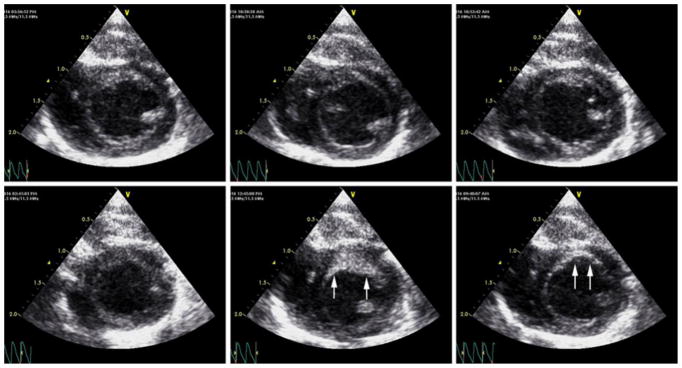
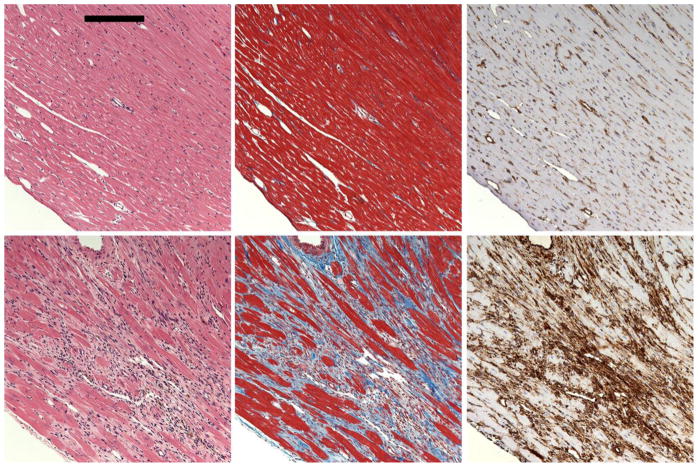
Ultrasound myocardial cavitation-enabled treatment was applied to the SS-16BN rat model of hypertrophic cardiomyopathy for proof of the principle underlying myocardial reduction therapy. A focused ultrasound transducer was targeted using 10-MHz imaging (10 S, GE Vivid 7) to the left ventricular wall of anesthetized rats in a warmed water bath. Pulse bursts of 4-MPa peak rarefactional pressure amplitude were intermittently triggered 1:8 heartbeats during a 10-min infusion of a microbubble suspension. Methylprednisolone was given to reduce initial inflammation, and Losartan was given to reduce fibrosis in the healing tissue. At 28 d post therapy, myocardial cavitation-enabled treatment significantly reduced the targeted wall thickness by 16.2% (p <0.01) relative to shams, with myocardial strain rate and endocardial displacement reduced by 34% and 29%, respectively, which are sufficient for therapeutic treatment. Premature electrocardiogram complexes and plasma troponin measurements were found to identify optimal and suboptimal treatment cohorts and would aid in achieving the desired impact. With clinical translation, myocardial cavitation-enabled treatment should fill the need for a new non-invasive hypertrophic cardiomyopathy therapy option.
Keywords: Cardiac fibrosis; Cardiac myocyte necrosis; Hypertrophic cardiomyopathy; Myocardial contrast echocardiography; Ultrasonic cavitation.
Copyright © 2018 World Federation for Ultrasound in Medicine and Biology. Published by Elsevier Inc. All rights reserved.
Figures




Similar articles
-
Multiple ultrasound cavitation-enabled treatments for myocardial reduction.J Ther Ultrasound. 2017 Nov 9;5:29. doi: 10.1186/s40349-017-0107-x. eCollection 2017. J Ther Ultrasound. 2017. PMID: 29152303 Free PMC article.
-
Maturation of Lesions Induced by Myocardial Cavitation-Enabled Therapy.Ultrasound Med Biol. 2016 Jul;42(7):1541-50. doi: 10.1016/j.ultrasmedbio.2016.02.006. Epub 2016 Apr 14. Ultrasound Med Biol. 2016. PMID: 27087693 Free PMC article.
-
Optimization of ultrasound parameters of myocardial cavitation microlesions for therapeutic application.Ultrasound Med Biol. 2014 Jun;40(6):1228-36. doi: 10.1016/j.ultrasmedbio.2014.01.001. Epub 2014 Mar 6. Ultrasound Med Biol. 2014. PMID: 24613640 Free PMC article.
-
Italian Society of Cardiovascular Echography (SIEC) Consensus Conference on the state of the art of contrast echocardiography.Ital Heart J. 2004 Apr;5(4):309-34. Ital Heart J. 2004. PMID: 15185894 Review.
-
Emerging pharmacologic and structural therapies for hypertrophic cardiomyopathy.Heart Fail Rev. 2017 Nov;22(6):879-888. doi: 10.1007/s10741-017-9648-x. Heart Fail Rev. 2017. PMID: 28856513 Review.
Cited by
-
Microbubble-Facilitated Ultrasound Catheter Ablation Causes Microvascular Damage and Fibrosis.Ultrasound Med Biol. 2021 Jan;47(1):131-138. doi: 10.1016/j.ultrasmedbio.2020.09.007. Epub 2020 Oct 20. Ultrasound Med Biol. 2021. PMID: 33092899 Free PMC article.
-
Role of Ultrasound-Based Therapies in Cardiovascular Diseases.Struct Heart. 2024 Jul 16;9(2):100349. doi: 10.1016/j.shj.2024.100349. eCollection 2025 Feb. Struct Heart. 2024. PMID: 40124079 Free PMC article. Review.
-
A Narrative Review of Current and Investigational Therapies in Hypertrophic Cardiomyopathy.Biomedicines. 2025 May 29;13(6):1327. doi: 10.3390/biomedicines13061327. Biomedicines. 2025. PMID: 40564046 Free PMC article. Review.
-
Numerical Assessment of Combustion Behavior and Emission Formations in an Ultrasonic-Assisted Ignition Engine.ACS Omega. 2023 Sep 22;8(39):36418-36434. doi: 10.1021/acsomega.3c05415. eCollection 2023 Oct 3. ACS Omega. 2023. PMID: 37810679 Free PMC article.
-
Multiple ultrasound cavitation-enabled treatments for myocardial reduction.J Ther Ultrasound. 2017 Nov 9;5:29. doi: 10.1186/s40349-017-0107-x. eCollection 2017. J Ther Ultrasound. 2017. PMID: 29152303 Free PMC article.
References
-
- Brown ML, Schaff HV, Dearani JA, Li Z, Nishimura RA, Ommen SR. Relationship between left ventricular mass, wall thickness, and survival after subaortic septal myectomy for hypertrophic obstructive cardiomyopathy. J Thorac Cardiovasc Surg. 2011;141:439–443. - PubMed
-
- Chao J, Zhang JJ, Lin KF, Chao L. Human kallikrein gene delivery attenuates hypertension, cardiac hypertrophy, and renal injury in Dahl salt-sensitive rats. Hum Gene Ther. 1998;9:21–31. - PubMed
-
- Crake C, Owen J, Smart S, Coviello C, Coussios CC, Carlisle R, Stride E. Enhancement and Passive Acoustic Mapping of Cavitation from Fluorescently Tagged Magnetic Resonance-Visible Magnetic Microbubbles In Vivo. Ultrasound Med Biol. 2016;42:3022–3036. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
