

A Comparative 68Ga-Citrate and 68Ga-Chloride PET/CT Imaging of Staphylococcus aureus Osteomyelitis in the Rat Tibia
- PMID: 29681785
- PMCID: PMC5845485
- DOI: 10.1155/2018/9892604
A Comparative 68Ga-Citrate and 68Ga-Chloride PET/CT Imaging of Staphylococcus aureus Osteomyelitis in the Rat Tibia
Abstract
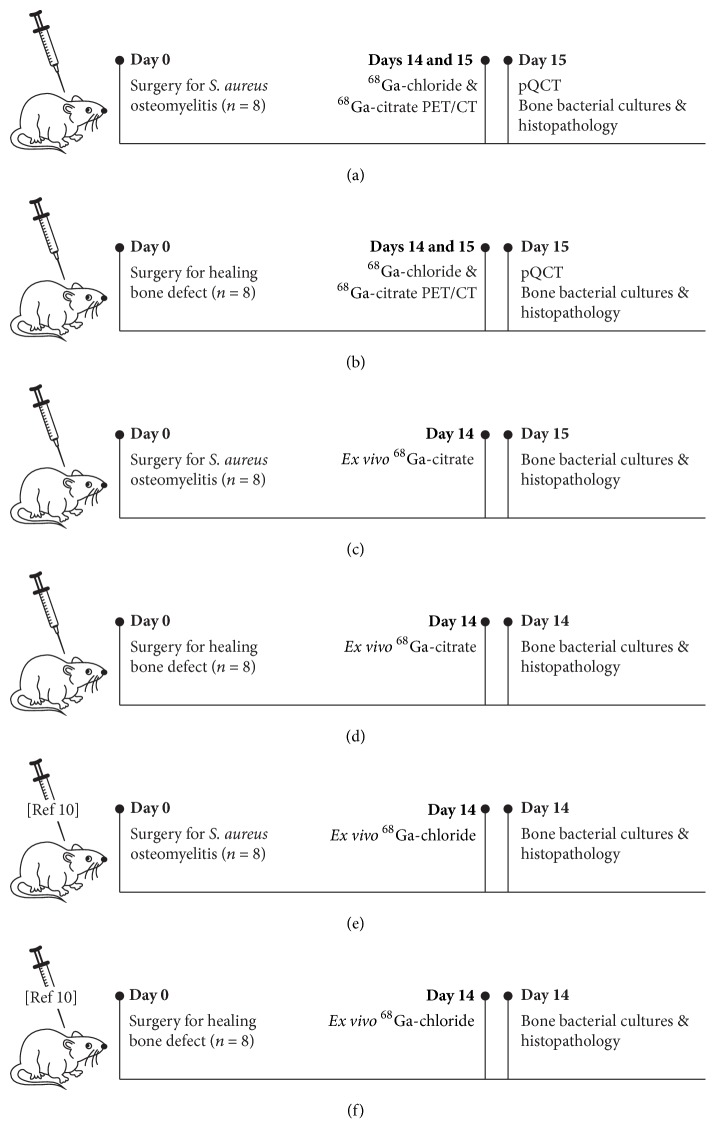
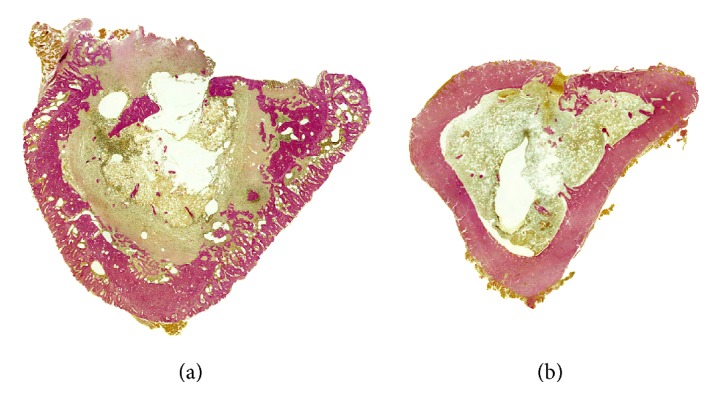
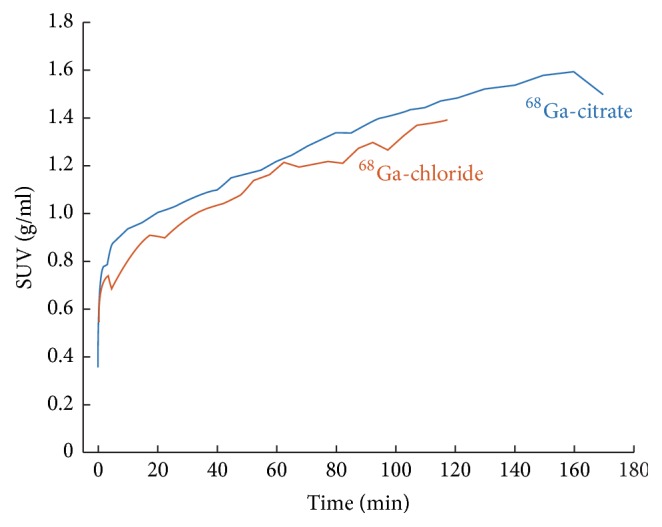
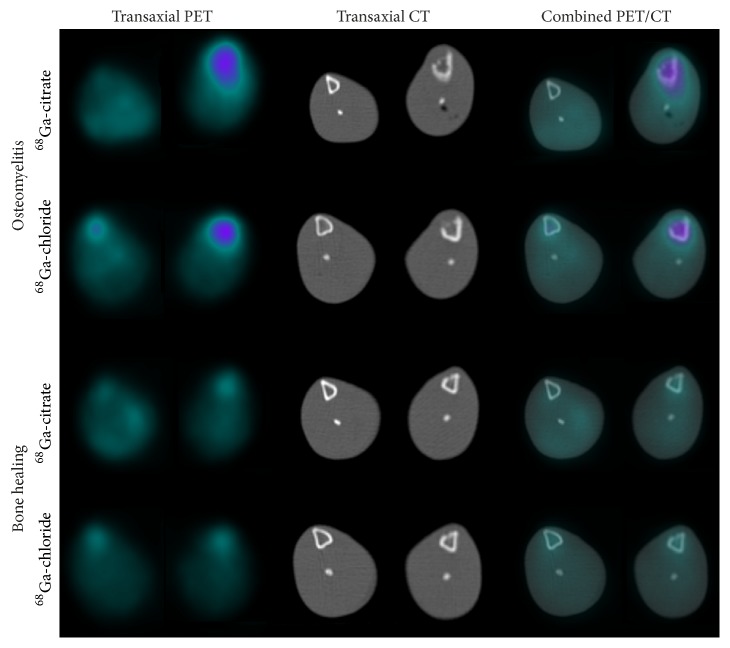
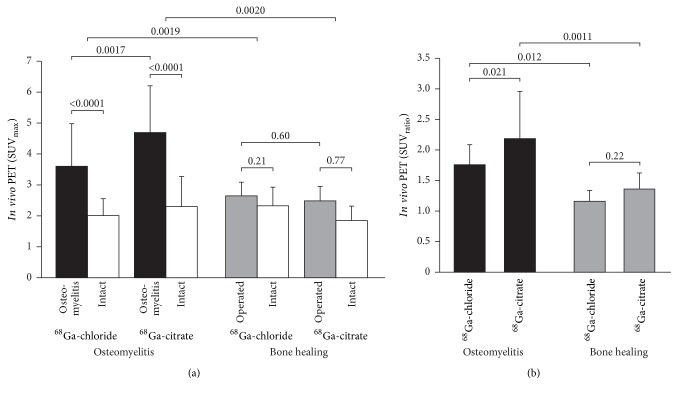
There may be some differences in the in vivo behavior of 68Ga-chloride and 68Ga-citrate leading to different accumulation profiles. This study compared 68Ga-citrate and 68Ga-chloride PET/CT imaging under standardized experimental models. Methods. Diffuse Staphylococcus aureus tibial osteomyelitis and uncomplicated bone healing rat models were used (n = 32). Two weeks after surgery, PET/CT imaging was performed on consecutive days using 68Ga-citrate or 68Ga-chloride, and tissue accumulation was confirmed by ex vivo analysis. In addition, peripheral quantitative computed tomography and conventional radiography were performed. Osteomyelitis was verified by microbiological analysis and specimens were also processed for histomorphometry. Results. In PET/CT imaging, the SUVmax of 68Ga-chloride and 68Ga-citrate in the osteomyelitic tibias (3.6 ± 1.4 and 4.7 ± 1.5, resp.) were significantly higher (P = 0.0019 and P = 0.0020, resp.) than in the uncomplicated bone healing (2.7 ± 0.44 and 2.5 ± 0.49, resp.). In osteomyelitic tibias, the SUVmax of 68Ga-citrate was significantly higher than the uptake of 68Ga-chloride (P = 0.0017). In animals with uncomplicated bone healing, no difference in the SUVmax of 68Ga-chloride or 68Ga-citrate was seen in the operated tibias. Conclusions. This study further corroborates the use of 68Ga-citrate for PET imaging of osteomyelitis.
Figures
References
-
- Termaat M. F., Raijmakers P. G. H. M., Scholten H. J., Barker F. C., Patka P., Haarman H. J. T. M. The accuracy of diagnostic imaging for the assessment of chronic osteomyelitis: a systematic review and meta-analysis. The Journal of Bone and Joint Surgery—American Volume. 2005;87(11):2464–2471. doi: 10.2106/jbjs.d.02691. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
