

Adult Versus Pediatric Tethered Cord Syndrome: Clinicoradiological Differences and its Management
- PMID: 29682019
- PMCID: PMC5898090
- DOI: 10.4103/1793-5482.228566
Adult Versus Pediatric Tethered Cord Syndrome: Clinicoradiological Differences and its Management
Abstract
Background: Dysraphic lesions in adults, presenting clinically as tethered cord syndrome (TCS), are relatively rare, and their optimal management remains controversial.
Patients and methods: We performed a retrospective analysis of our pediatric database over a period of last 7 years to focus on the adult TCS. Our aim was to determine the clinicoradiological and etiopathological differences between adult and pediatric patients as well as to determine the results of surgery in adult TCS.
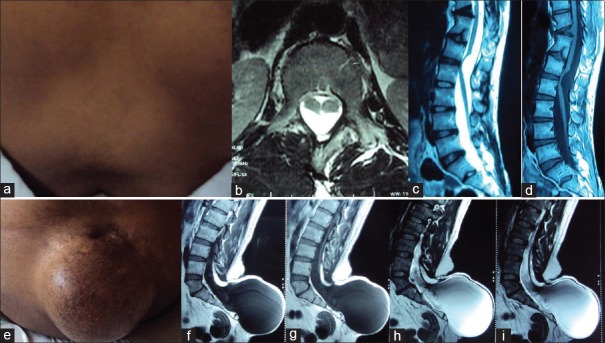
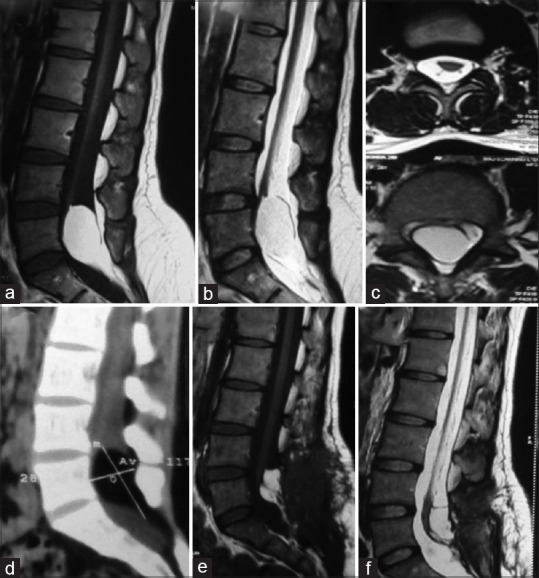
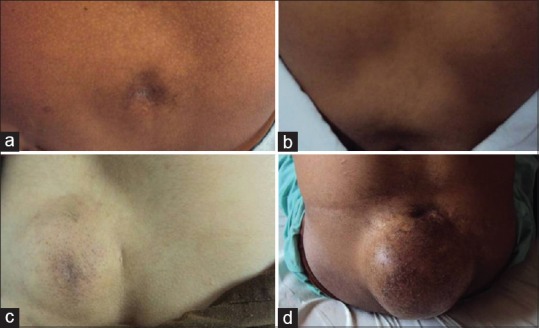
Results: Adult spinal dysraphisms constituted 15.4% of our patients (20 out of 130). Motor weakness, sphincteric dysfunction, and backache (n = 13, 65.0% each) predominated in adults unlike children who presented with subcutaneous swellings (n = 74, 67.6%) followed by motor weakness (n = 40, 46.4%), backache being reported by only three patients. The different pathologic substrates underlying adult dysraphisms were lipomeningocele (n = 8), split cord malformation (total = 7; Type 1: n = 5; Type 2: n = 2), dermal sinus (n = 2), and fatty filum (n = 3). On the other hand, meningomyelocele/meningocele (61, 54.9%) followed by split cord malformation Type 1 and 2 (n = 29, 26.1%) predominated in children. The radiological differences between the two groups were a higher incidence of vertebral body defects (hemivertebrae and butterfly vertebrae) and lack of intracranial anomalies in adults. At a mean follow-up of 20.5 months, the most common symptoms to improve following detethering were pain (11 out of 13, 84.6%) followed by motor weakness (six out of 13, 56.2%) and sphincteric control (7 out of 13, 53.8%).
Conclusion: Most common symptoms to improve following detethering in adult TCS were pain followed by motor weakness. The major radiological differences between these two groups were a higher incidence of vertebral body defects (hemivertebrae and butterfly vertebrae) and lack of intracranial anomalies in adults.
Keywords: Adult spinal dysraphism; lipomyelomeningocele; split cord malformation; tethered cord syndrome.
Conflict of interest statement
There are no conflicts of interest.
Figures

Similar articles
-
Congenital tethered spinal cord syndrome in adults.J Neurosurg. 1998 Jun;88(6):958-61. doi: 10.3171/jns.1998.88.6.0958. J Neurosurg. 1998. PMID: 9609288
-
Surgical management of tethered cord syndrome in adults: indications, techniques, and long-term outcomes in 60 patients.J Neurosurg Spine. 2006 Feb;4(2):123-31. doi: 10.3171/spi.2006.4.2.123. J Neurosurg Spine. 2006. PMID: 16506479
-
Tethered cord syndrome and transitional vertebrae.Surg Radiol Anat. 2020 Feb;42(2):111-119. doi: 10.1007/s00276-019-02341-5. Epub 2019 Sep 19. Surg Radiol Anat. 2020. PMID: 31538247
-
Tethered cord syndrome: a review of the literature from embryology to adult presentation.Neurosurg Focus. 2010 Jul;29(1):E1. doi: 10.3171/2010.3.FOCUS1079. Neurosurg Focus. 2010. PMID: 20593997 Review.
-
Split cord malformation and tethered cord syndrome: case series with long-term follow-up and literature review.Childs Nerv Syst. 2021 Apr;37(4):1301-1306. doi: 10.1007/s00381-020-04978-9. Epub 2020 Nov 26. Childs Nerv Syst. 2021. PMID: 33242106 Review.
Cited by
-
Cerebrospinal Fluid Leaks and Healthcare Costs Associated With Tethered Cord Release and Filum Terminale Sectioning.Cureus. 2025 Mar 5;17(3):e80102. doi: 10.7759/cureus.80102. eCollection 2025 Mar. Cureus. 2025. PMID: 40190864 Free PMC article.
-
Application of neurophysiological monitoring during tethered cord release in children.Childs Nerv Syst. 2024 Sep;40(9):2921-2927. doi: 10.1007/s00381-024-06483-9. Epub 2024 Jun 8. Childs Nerv Syst. 2024. PMID: 38850295 Free PMC article.
-
Pediatric tethered cord release: an epidemiological and postoperative complication analysis.J Spine Surg. 2019 Sep;5(3):337-350. doi: 10.21037/jss.2019.09.02. J Spine Surg. 2019. PMID: 31663045 Free PMC article.
-
Lipomeningocele with Tethered Cord Syndrome in an Adult: A Case Report.JNMA J Nepal Med Assoc. 2023 Jul;61(263):620-622. doi: 10.31729/jnma.8220. Epub 2023 Jul 30. JNMA J Nepal Med Assoc. 2023. PMID: 40802714 Free PMC article.
-
Disparities in indications and outcomes reporting for pediatric tethered cord surgery: The need for a standardized outcome assessment tool.Childs Nerv Syst. 2024 Apr;40(4):1111-1120. doi: 10.1007/s00381-023-06246-y. Epub 2023 Dec 11. Childs Nerv Syst. 2024. PMID: 38072858 Free PMC article.
References
-
- Yamada S, Won DJ. What is the true tethered cord syndrome? Childs Nerv Syst. 2007;23:371–5. - PubMed
-
- Hoffman HJ, Hendrick EB, Humphreys RP. The tethered spinal cord: Its protean manifestations, diagnosis and surgical correction. Childs Brain. 1976;2:145–55. - PubMed
-
- Yamada S, Zinke DE, Sanders D. Pathophysiology of “tethered cord syndrome”. J Neurosurg. 1981;54:494–503. - PubMed
-
- Klekamp J. Tethered cord syndrome in adults. J Neurosurg Spine. 2011;15:258–70. - PubMed
-
- Hüttmann S, Krauss J, Collmann H, Sörensen N, Roosen K. Surgical management of tethered spinal cord in adults: Report of 54 cases. J Neurosurg. 2001;95(2 Suppl):173–8. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources