

Diagnostic intervals and pancreatic ductal adenocarcinoma (PDAC) resectability: a single-center retrospective analysis
- PMID: 29683142
- PMCID: PMC5909699
- DOI: 10.21037/apc.2018.02.01
Diagnostic intervals and pancreatic ductal adenocarcinoma (PDAC) resectability: a single-center retrospective analysis
Abstract
Background: Pancreatic ductal adenocarcinoma (PDAC) often presents with nonspecific symptoms and the workup is not standardized. To study the impact of delays in diagnosis and in the initiation of treatment, we investigated the relationship between length of diagnostic intervals and surgical resectability.
Methods: We performed a retrospective chart review of patients evaluated for PDAC at Johns Hopkins in 2014. Data were collected on the patient (date of first symptoms-first medical appointment), diagnostic (first medical appointment-diagnosis of PDAC), and treatment (diagnosis of PDAC-1st day of treatment) time intervals, and the upfront treatment received. Asymptomatic patients diagnosed incidentally, or for whom records were incomplete, were excluded from analysis.
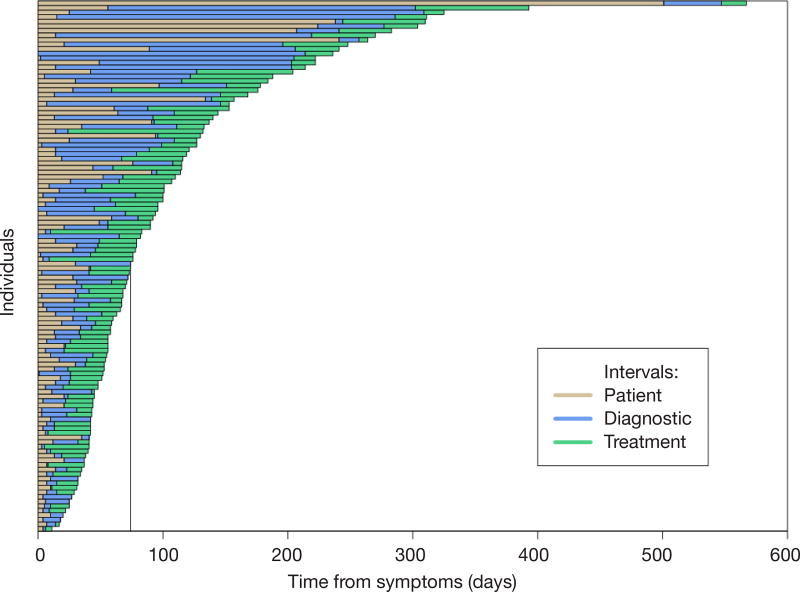
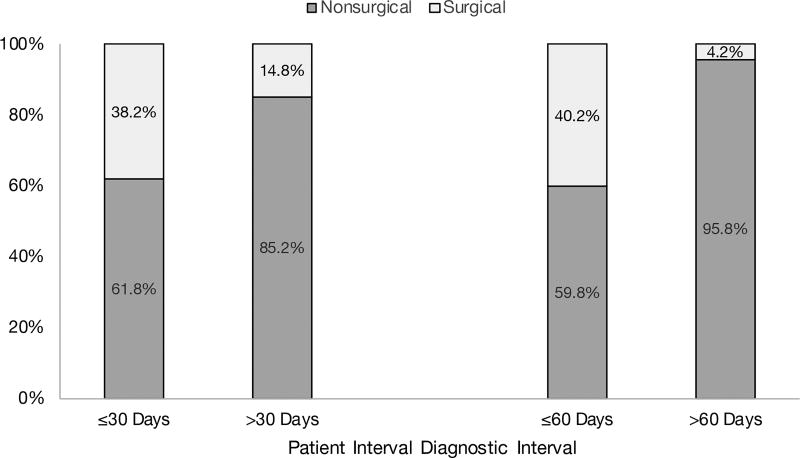
Results: Of 453 charts reviewed, 116 patients met inclusion criteria. The median patient interval was 14 days [interquartile range (IQR): 6-30 days], the median diagnostic interval was 22 days (IQR: 8-46 days), and the median treatment interval was 26 days (IQR: 15-35 days). Thirty-eight patients (33%) received upfront surgery and 78 (67%) received nonsurgical treatment. After adjusting for multiple factors, the odds of receiving surgery significantly increased for individuals with a patient interval of 30 days or less [adjusted odds ratio (aOR): 3.41; 95% confidence interval (CI): 1.08-13.20; P=0.050] and with a diagnostic interval of 60 days or less (aOR: 15.68; 95% CI: 2.95-291.00, P=0.009).
Conclusions: A patient interval less than 1 month and a diagnostic interval less than 2 months for symptomatic PDAC are associated with increased odds of upfront surgical resection. These data provide initial evidence that reducing diagnostic delays may lead to improved outcomes in PDAC.
Keywords: Pancreatic ductal adenocarcinoma (PDAC); diagnostic delay; diagnostic intervals; surgical resection.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Gress FG, Hawes RH, Savides TJ, et al. Role of EUS in the preoperative staging of pancreatic cancer: a large single-center experience. Gastrointest Endosc. 1999;50:786–91. - PubMed
-
- Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus Gemcitabine for Metastatic Pancreatic Cancer. N Engl J Med. 2011;364:1817–25. - PubMed
-
- Callery MP, Chang KJ, Fishman EK, et al. Pretreatment assessment of resectable and borderline resectable pancreatic cancer: expert consensus statement. Ann Surg Oncol. 2009;16:1727–33. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous