

Risk of recurrence and death in patients with breast cancer after delayed deep inferior epigastric perforator flap reconstruction
- PMID: 29683203
- PMCID: PMC6174948
- DOI: 10.1002/bjs.10866
Risk of recurrence and death in patients with breast cancer after delayed deep inferior epigastric perforator flap reconstruction
Abstract
Background: Postmastectomy reconstruction using a deep inferior epigastric perforator (DIEP) flap is increasingly being performed in patients with breast cancer. The procedure induces extensive tissue trauma, and it has been hypothesized that the release of growth factors, angiogenic agonists and immunomodulating factors may reactivate dormant micrometastasis. The aim of the present study was to estimate the risk of breast cancer recurrence in patients undergoing DIEP flap reconstruction compared with that in patients treated with mastectomy alone.
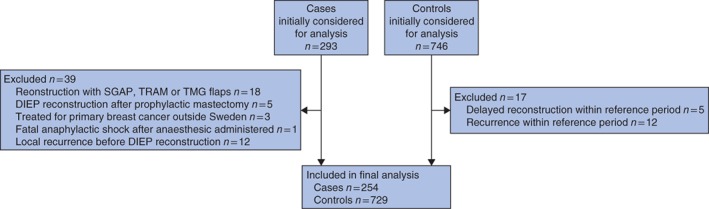
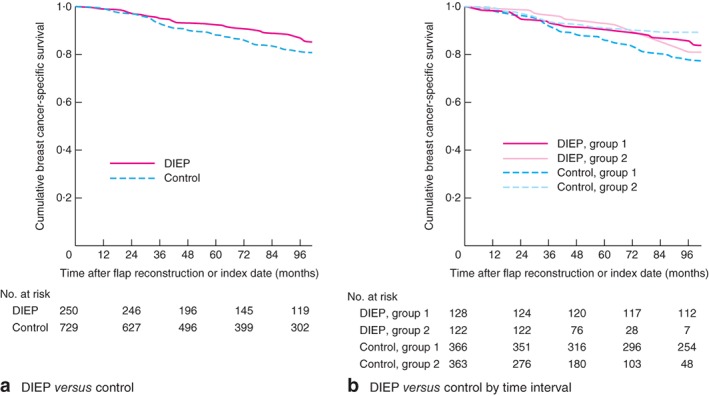
Methods: Each patient who underwent delayed DIEP flap reconstruction at Karolinska University Hospital, Sweden, between 1999 and 2013, was compared with up to four controls with breast cancer who did not receive a DIEP flap. The control patients were selected using incidence density matching with respect to age, tumour and nodal status, neoadjuvant therapy and year of mastectomy. The primary endpoint was breast cancer-specific survival. Survival analysis was carried out using Kaplan-Meier survival estimates and Cox proportional hazard regression analysis.
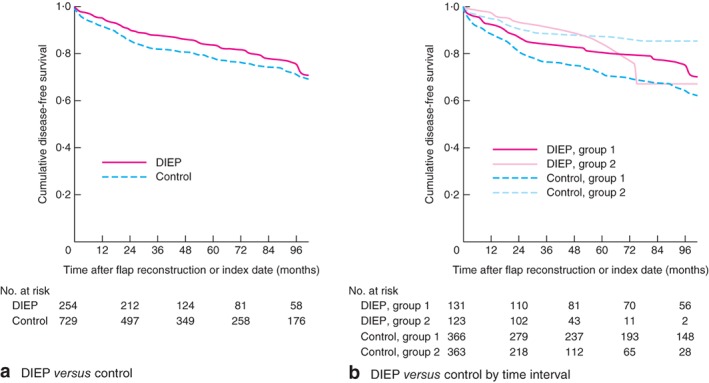
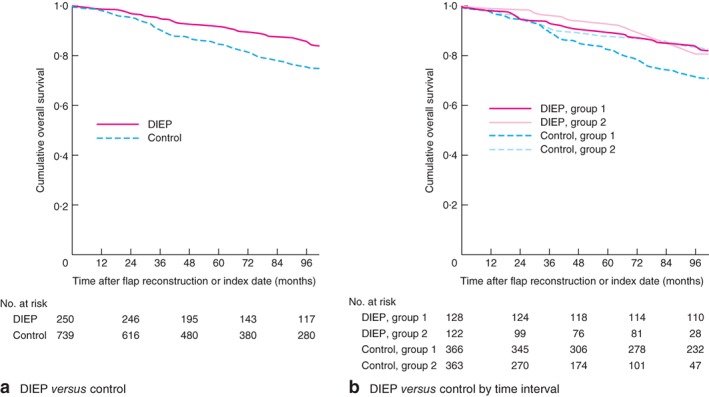
Results: The analysis included 250 patients who had 254 DIEP flap reconstructions and 729 control patients. Median follow-up was 89 and 75 months respectively (P = 0·053). Breast cancer recurrence developed in 50 patients (19·7 per cent) in the DIEP group and 174 (23·9 per cent) in the control group (P = 0·171). The 5-year breast cancer-specific survival rate was 92·0 per cent for patients with a DIEP flap and 87·9 per cent in controls (P = 0·032). Corresponding values for 5-year overall survival were 91·6 and 84·7 per cent (P < 0·001). After adjustment for tumour and patient characteristics and treatment, patients without DIEP flap reconstruction had significantly lower overall but not breast cancer-specific survival.
Conclusion: The present findings do not support the hypothesis that patients with breast cancer undergoing DIEP flap reconstruction have a higher rate of breast cancer recurrence than those who have mastectomy alone.
© 2018 The Authors. BJS published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures
References
-
- Zhong T, Hu J, Bagher S, Vo A, O'Neill AC, Butler K et al A comparison of psychological response, body image, sexuality, and quality of life between immediate and delayed autologous tissue breast reconstruction: a prospective long‐term outcome study. Plast Reconstr Surg 2016; 138: 772–780. - PubMed
-
- Juhl AA, Christensen S, Zachariae R, Damsgaard TE. Unilateral breast reconstruction after mastectomy – patient satisfaction, aesthetic outcome and quality of life. Acta Oncol 2017; 56: 225–231. - PubMed
-
- Taghizadeh R, Moustaki M, Harris S, Roblin P, Farhadi J. Does post‐mastectomy radiotherapy affect the outcome and prevalence of complications in immediate DIEP breast reconstruction? A prospective cohort study. J Plast Reconstr Aesthet Surg 2015; 68: 1379–1385. - PubMed
-
- Clarke‐Pearson EM, Chadha M, Dayan E, Dayan JH, Samson W, Sultan MR et al Comparison of irradiated versus nonirradiated DIEP flaps in patients undergoing immediate bilateral DIEP reconstruction with unilateral postmastectomy radiation therapy (PMRT). Ann Plast Surg 2013; 71: 250–254. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
