

Economic Analysis of Neoadjuvant Chemotherapy Versus Primary Debulking Surgery for Advanced Epithelial Ovarian Cancer Using an Aggressive Surgical Paradigm
- PMID: 29683880
- PMCID: PMC6033676
- DOI: 10.1097/IGC.0000000000001271
Economic Analysis of Neoadjuvant Chemotherapy Versus Primary Debulking Surgery for Advanced Epithelial Ovarian Cancer Using an Aggressive Surgical Paradigm
Abstract
Objectives: Neoadjuvant chemotherapy (NACT) versus primary debulking surgery (PDS) for advanced epithelial ovarian cancer (AEOC) remains controversial in the United States. Generalizability of existing trial results has been criticized because of less aggressive debulking procedures than commonly used in the United States. As a result, economic evaluations using input data from these trials may not accurately reflect costs and outcomes associated with more aggressive primary surgery. Using data from an ongoing trial performing aggressive debulking, we investigated the cost-effectiveness and cost-utility of NACT versus PDS for AEOC.
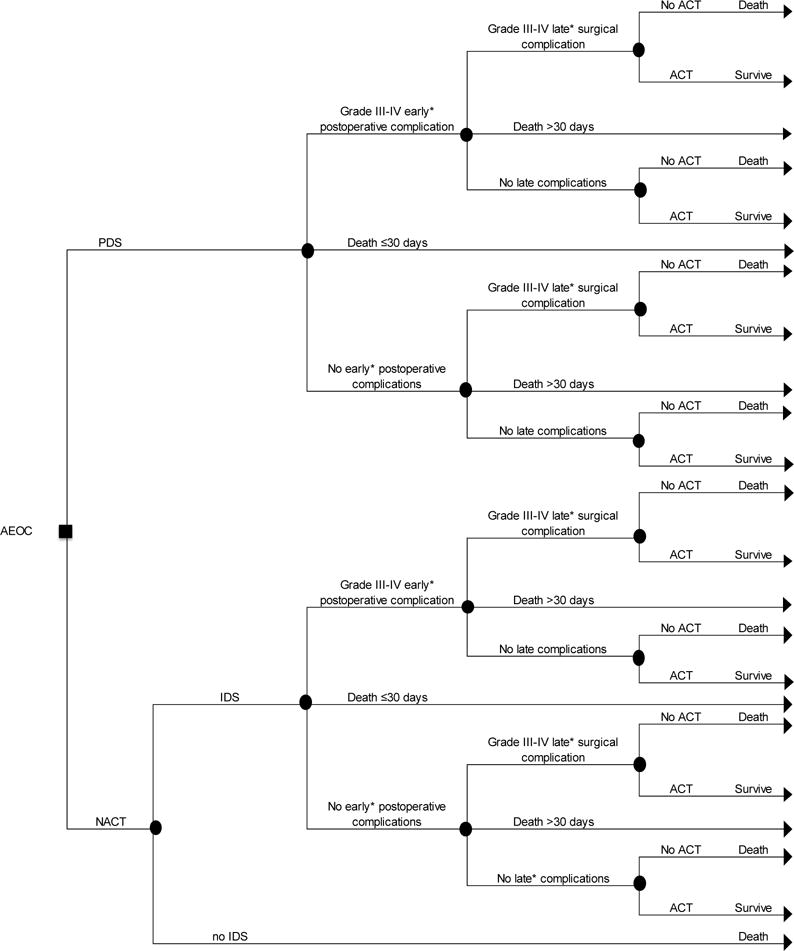
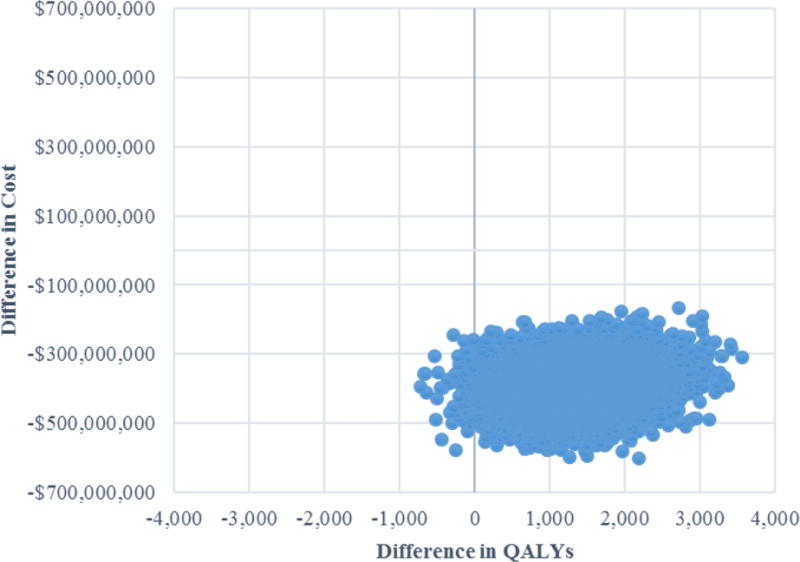
Methods: A decision tree model was constructed to estimate differences in short-term outcomes and costs for a hypothetical cohort of 15,000 AEOC patients (US annual incidence of AEOC) treated with NACT versus PDS over a 1-year time horizon from a Medicare payer perspective. Outcomes included costs per cancer-related death averted, life-years and quality-adjusted life-years (QALYs) gained. Base-case probabilities, costs, and utilities were based on the Surgical Complications Related to Primary or Interval Debulking in Ovarian Neoplasms trial. Base-case analyses assumed equivalent survival; threshold analysis estimated the maximum survival difference that would result in NACT being cost-effective at $50,000/QALY and $100,000/QALY willingness-to-pay thresholds. Probabilistic sensitivity analysis was used to characterize model uncertainty.
Results: Compared with PDS, NACT was associated with $142 million in cost savings, 1098 fewer cancer-related deaths, and 1355 life-years and 1715 QALYs gained, making it the dominant treatment strategy for all outcomes. In sensitivity analysis, NACT remained dominant in 99.3% of simulations. Neoadjuvant chemotherapy remained cost-effective at $50,000/QALY and $100,000/QALY willingness-to-pay thresholds if survival differences were less than 2.7 and 1.4 months, respectively.
Conclusions: In the short term, NACT is cost-saving with improved outcomes. However, if PDS provides a longer-term survival advantage, it may be cost-effective. Research is needed on the role of patient preferences in tradeoffs between survival and quality of life.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66:7–30. - PubMed
-
-
SEER Stat Fact Sheets: Ovarian Cancer. National Cancer Institute Surveillance, Epidemiology, and End Results.
-
-
- Aletti GD, Dowdy SC, Gostout BS, Jones MB, Stanhope CR, Wilson TO, et al. Aggressive surgical effort and improved survival in advanced-stage ovarian cancer. Obstet Gynecol. 2006;107:77–85. - PubMed
-
- Aletti GD, Dowdy SC, Podratz KC, Cliby WA. Relationship among surgical complexity, short-term morbidity, and overall survival in primary surgery for advanced ovarian cancer. Am J Obstet Gynecol. 2007;197:676.e1–7. - PubMed
-
- Winter WE, 3rd, Maxwell GL, Tian C, Carlson JW, Ozols RF, Rose PG, et al. Prognostic factors for stage III epithelial ovarian cancer: a Gynecologic Oncology Group Study. J Clin Oncol. 2007;25:3621–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
