

Weekends-off efavirenz-based antiretroviral therapy in HIV-infected children, adolescents and young adults (BREATHER): Extended follow-up results of a randomised, open-label, non-inferiority trial
- PMID: 29684092
- PMCID: PMC5912750
- DOI: 10.1371/journal.pone.0196239
Weekends-off efavirenz-based antiretroviral therapy in HIV-infected children, adolescents and young adults (BREATHER): Extended follow-up results of a randomised, open-label, non-inferiority trial
Abstract
Background: Weekends off antiretroviral therapy (ART) may help engage HIV-1-infected young people facing lifelong treatment. BREATHER showed short cycle therapy (SCT; 5 days on, 2 days off ART) was non-inferior to continuous therapy (CT) over 48 weeks. Planned follow-up was extended to 144 weeks, maintaining original randomisation.
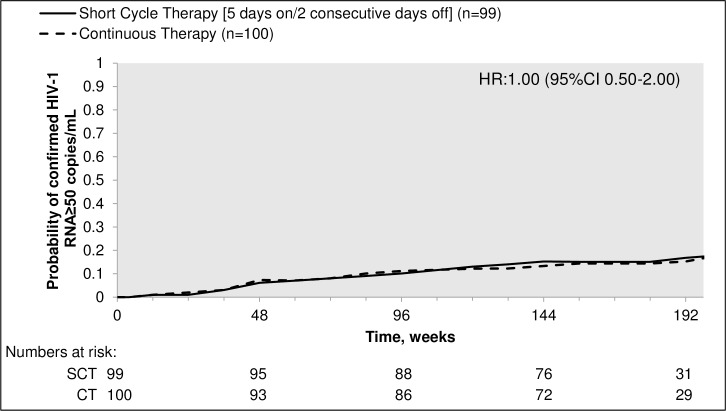
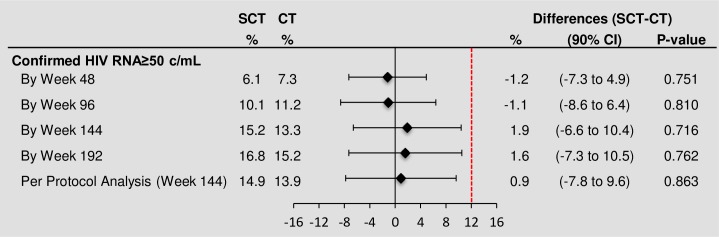
Methods: BREATHER was an open-label, non-inferiority trial. Participants aged 8-24yrs with virological suppression on efavirenz-based first-line ART were randomised 1:1, stratified by age and African/non-African sites, to remain on CT or change to SCT. The Kaplan-Meier method was used to estimate the proportion of participants with viral rebound (confirmed VL≥50 copies/mL) under intent-to-treat at 48 weeks (primary outcome), and in extended follow-up at 96, 144, and 192 weeks. SCT participants returned to CT following viral rebound, 3 VL blips or discontinuation of efavirenz.
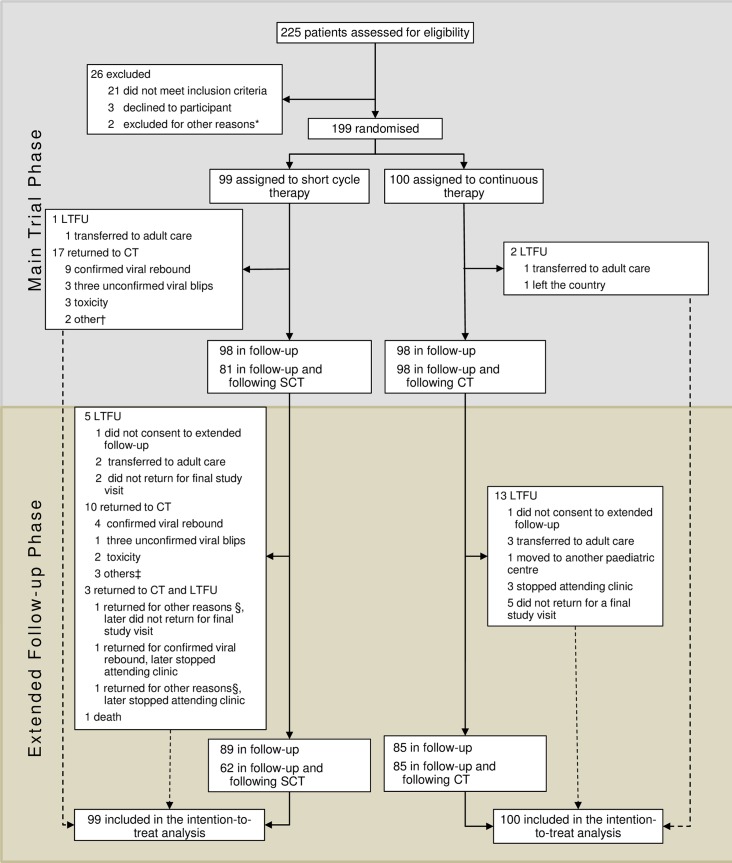
Findings: Of 199 participants (99 SCT, 100 CT), 97 per arm consented to extended follow-up. Median follow-up was 185.3 weeks (IQR 160.9-216.1). 69 (70%) SCT participants remained on SCT at last follow-up. 105 (53%) were male, baseline median age 14 years (IQR 12-18), median CD4 count 735 cells/μL (IQR 576-968). 16 SCT and 16 CT participants had confirmed VL≥50 copies/mL by the end of extended follow-up (HR 1.00, 95% CI 0.50-2.00). Estimated difference in percentage with viral rebound (SCT minus CT) by week 144 was 1.9% (90% CI -6.6-10.4; p = 0.72) and was similar in a per-protocol analysis. There were no significant differences between arms in proportions of participants with grade 3/4 adverse events (18 SCT vs 16 CT participants; p = 0.71) or ART-related adverse events (10 vs 12; p = 0.82). 20 versus 8 serious adverse events (SAEs) were reported in 16 SCT versus 4 CT participants, respectively (p = 0.005 comparing proportions between groups; incidence rate ratio 2.49, 95%CI 0.71-8.66, p = 0.15). 75% of SAEs (15 SCT, 6 CT) were hospitalisations for a wide range of conditions. 3 SCT and 6 CT participants switched to second-line ART following viral failure (p = 0.50).
Conclusions: Sustainable non-inferiority of virological suppression in young people was shown for SCT versus CT over median 3.6 years. Standard-dose efavirenz-based SCT is a viable option for virologically suppressed HIV-1 infected young people on first-line ART with 3-monthly VL monitoring.
Trial registration: EudraCT 2009-012947-40 ISRCTN 97755073 ClinicalTrials.gov NCT01641016.
Conflict of interest statement
Figures
References
-
- Joint United Nations Programme on HIV/AIDS (UNAIDS). UNAIDS 2016 estimates Geneva: UNAIDS; 2016. Available from: http://aidsinfo.unaids.org/.
-
- Joint United Nations Programme on HIV/AIDS (UNAIDS). Get on the fast-track—the life-cycle approach to HIV 2016. Available from: http://www.unaids.org/sites/default/files/media_asset/Get-on-the-Fast-Tr...
-
- Nachega JB, Hislop M, Nguyen H, Dowdy DW, Chaisson RE, Regensberg L, et al. Antiretroviral therapy adherence, virologic and immunologic outcomes in adolescents compared with adults in southern Africa. Journal of acquired immune deficiency syndromes (1999). 2009;51(1):65–71. doi: 10.1097/QAI.0b013e318199072e ; PubMed Central PMCID: PMC2674125. - DOI - PMC - PubMed
-
- Evans D, Menezes C, Mahomed K, Macdonald P, Untiedt S, Levin L, et al. Treatment outcomes of HIV-infected adolescents attending public-sector HIV clinics across Gauteng and Mpumalanga, South Africa. AIDS research and human retroviruses. 2013;29(6):892–900. doi: 10.1089/AID.2012.0215 ; PubMed Central PMCID: PMC3653371. - DOI - PMC - PubMed
-
- Auld AF, Agolory SG, Shiraishi RW, Wabwire-Mangen F, Kwesigabo G, Mulenga M, et al. Antiretroviral therapy enrollment characteristics and outcomes among HIV-infected adolescents and young adults compared with older adults—seven African countries, 2004–2013. MMWR Morbidity and mortality weekly report. 2014;63(47):1097–103. . - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
