

Association Between Proportion of Nuclei With High Chromatin Entropy and Prognosis in Gynecological Cancers
- PMID: 29684152
- PMCID: PMC6292794
- DOI: 10.1093/jnci/djy063
Association Between Proportion of Nuclei With High Chromatin Entropy and Prognosis in Gynecological Cancers
Abstract
Background: Nuclear texture analysis measuring differences in chromatin structure has provided prognostic biomarkers in several cancers. There is a need for improved cell-by-cell chromatin analysis to detect nuclei with highly disorganized chromatin. The purpose of this study was to develop a method for detecting nuclei with high chromatin entropy and to evaluate the association between the presence of such deviating nuclei and prognosis.
Methods: A new texture-based biomarker that characterizes each cancer based on the proportion of high-chromatin entropy nuclei (<25% vs ≥25%) was developed on a discovery set of 175 uterine sarcomas. The prognostic impact of this biomarker was evaluated on a validation set of 179 uterine sarcomas, as well as on independent validation sets of 246 early-stage ovarian carcinomas and 791 endometrial carcinomas. More than 1 million images of nuclei stained for DNA were included in the study. All statistical tests were two-sided.
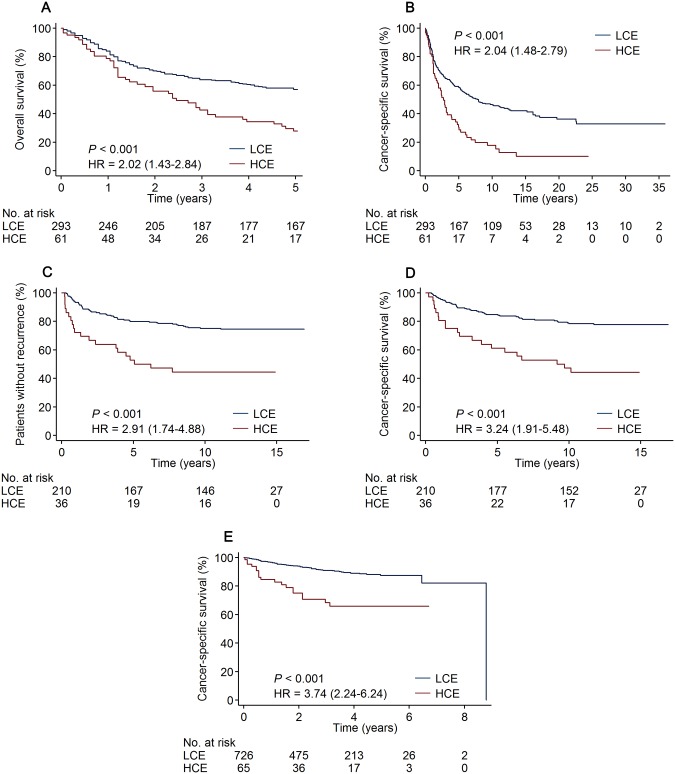
Results: An increased proportion of high-chromatin entropy nuclei was associated with poor clinical outcome. The biomarker predicted five-year overall survival for uterine sarcoma patients with a hazard ratio (HR) of 2.02 (95% confidence interval [CI] = 1.43 to 2.84), time to recurrence for ovarian cancer patients (HR = 2.91, 95% CI = 1.74 to 4.88), and cancer-specific survival for endometrial cancer patients (HR = 3.74, 95% CI = 2.24 to 6.24). Chromatin entropy was an independent prognostic marker in multivariable analyses with clinicopathological parameters (HR = 1.81, 95% CI = 1.21 to 2.70, for sarcoma; HR = 1.71, 95% CI = 1.01 to 2.90, for ovarian cancer; and HR = 2.03, 95% CI = 1.19 to 3.45, for endometrial cancer).
Conclusions: A novel method detected high-chromatin entropy nuclei, and an increased proportion of such nuclei was associated with poor prognosis. Chromatin entropy supplemented existing prognostic markers in multivariable analyses of three gynecological cancer cohorts.
Figures



References
-
- Hanahan D, Weinberg RA.. Hallmarks of cancer: The next generation. Cell. 2011;1445:646–674. - PubMed
-
- Jamal-Hanjani M, Wilson GA, McGranahan N, et al. Tracking the evolution of non–small-cell lung cancer. N Engl J Med. 2017;376:2109–2121. - PubMed
-
- Danielsen HE, Pradhan M, Novelli M.. Revisiting tumor aneuploidy – the place of ploidy assessment in the molecular area. Nat Rev Clin Oncol. 2016;135:291–304. - PubMed
-
- Wolffe AP. Chromatin remodeling: Why it is important in cancer. Oncogene. 2001;2024:2988–2990. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
