

Traumatic cardiac arrest in Sweden 1990-2016 - a population-based national cohort study
- PMID: 29685180
- PMCID: PMC5913805
- DOI: 10.1186/s13049-018-0500-7
Traumatic cardiac arrest in Sweden 1990-2016 - a population-based national cohort study
Abstract
Background: Trauma is a main cause of death among young adults worldwide. Patients experiencing a traumatic cardiac arrest (TCA) certainly have a poor prognosis but population-based studies are sparse. Primarily to describe characteristics and 30-day survival following a TCA as compared with a medical out-of-hospital cardiac arrest (medical CA).
Methods: A cohort study based on data from the nationwide, prospective population-based Swedish Registry for Cardiopulmonary Resuscitation (SRCR), a medical cardiac arrest registry, between 1990 and 2016. The definition of a TCA in the SRCR is a patient who is unresponsive with apnoea where cardiopulmonary resuscitation and/or defibrillation have been initiated and in whom the Emergency Medical Services (EMS, mainly a nurse-based system) reported trauma as the aetiology. Outcome was overall 30-day survival. Descriptive statistics as well as multivariable logistic regression models were used.
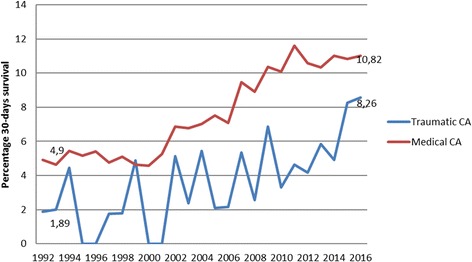
Results: In all, between 1990 and 2016, 1774 (2.4%) cases had a TCA and 72,547 had a medical CA. Overall 30-day survival gradually increased over the years, and was 3.7% for TCAs compared to 8.2% following a medical CA (p < 0.01). Among TCAs, factors associated with a higher 30-day survival were bystander witnessed and having a shockable initial rhythm (adjusted OR 2.67, 95% C.I. 1.15-6.22 and OR 8.94 95% C.I. 4.27-18.69, respectively).
Discussion: Association in registry-based studies do not imply causality but TCA had short time intervals in the chain of survival as well as high rates of bystander-CPR.
Conclusion: In a medical CA registry like ours, prevalence of TCAs is low and survival is poor. Registries like ours might not capture the true incidence. However, many individuals do survive and resuscitation in TCAs should not be seen futile.
Keywords: OHCA; Prevalence; Resuscitation; TCA; Trauma.
Conflict of interest statement
Ethics approval and consent to participate
This was a study based on register data. Survivors are informed about their participation and can afterwards withdraw their inclusion in the registry. Since the start of the registry in 1990 only a handful of patients have withdrawn their participation. Deceased patients are included without consent. The Regional Ethical Review Board in Stockholm, Sweden approved the study, Dnr 2013/1959-31/4.
Consent for publication
The manuscript does not contain individual person’s data, therefore consent for publications is not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
