

Increased cardiovascular risk in rheumatoid arthritis: mechanisms and implications
- PMID: 29685876
- PMCID: PMC6889899
- DOI: 10.1136/bmj.k1036
Increased cardiovascular risk in rheumatoid arthritis: mechanisms and implications
Abstract
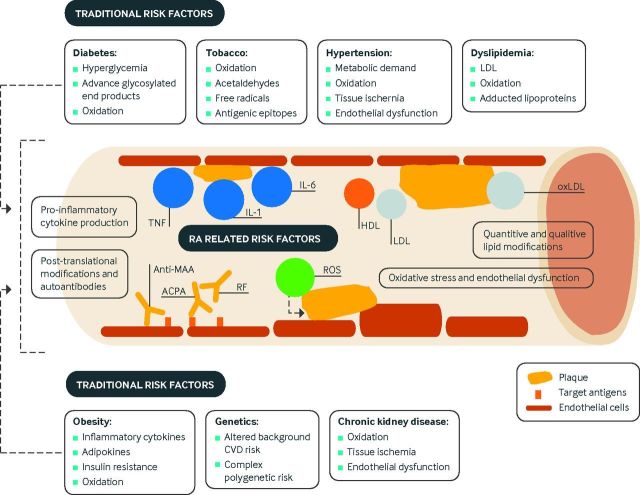
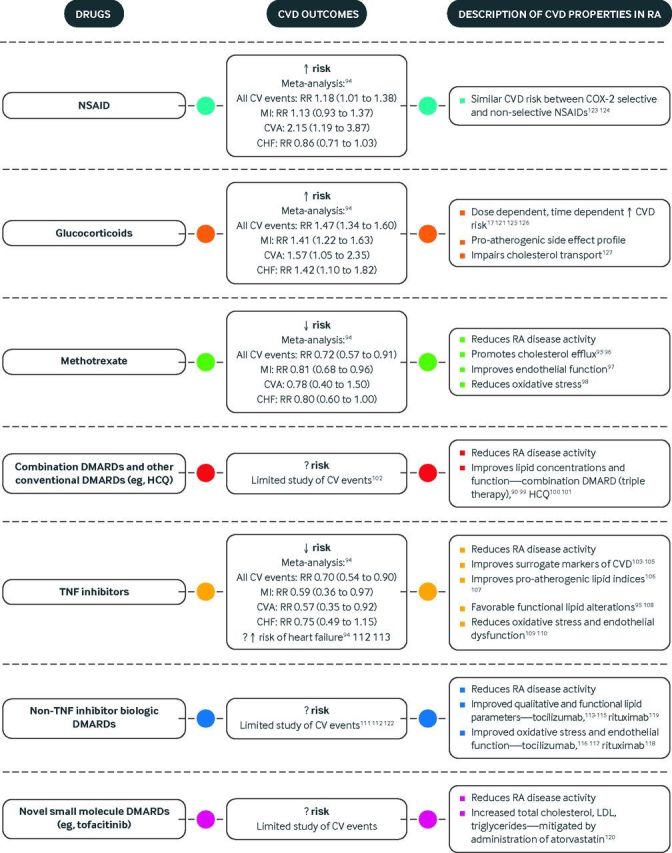
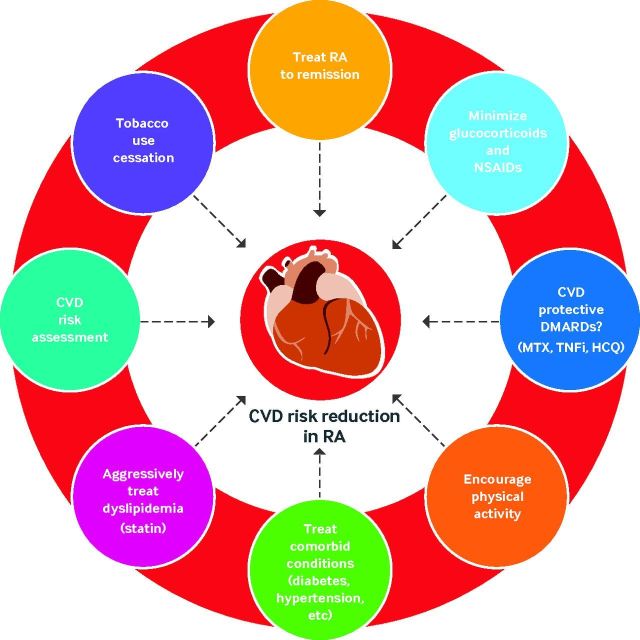
Rheumatoid arthritis is a systemic autoimmune disease characterized by excess morbidity and mortality from cardiovascular disease. Mechanisms linking rheumatoid arthritis and cardiovascular disease include shared inflammatory mediators, post-translational modifications of peptides/proteins and subsequent immune responses, alterations in the composition and function of lipoproteins, increased oxidative stress, and endothelial dysfunction. Despite a growing understanding of these mechanisms and their complex interplay with conventional cardiovascular risk factors, optimal approaches of risk stratification, prevention, and treatment in the context of rheumatoid arthritis remain unknown. A multifaceted approach to reduce the burden posed by cardiovascular disease requires optimal management of traditional risk factors in addition to those intrinsic to rheumatoid arthritis such as increased disease activity. Treatments for rheumatoid arthritis seem to exert differential effects on cardiovascular risk as well as the mechanisms linking these conditions. More research is needed to establish whether preferential rheumatoid arthritis therapies exist in terms of prevention of cardiovascular disease. Ultimately, understanding the unique mechanisms for cardiovascular disease in rheumatoid arthritis will aid in risk stratification and the identification of novel targets for meaningful reduction of cardiovascular risk in this patient population.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: We have read and understood the BMJ policy on declaration of interests and declare the following interests: TRM serves as a consultant for Pfizer.
Figures
References
-
- Sokka T, Abelson B, Pincus T. Mortality in rheumatoid arthritis: 2008 update. Clin Exp Rheumatol 2008;26(Suppl 51):S35-61. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical