

Analysis of Clinical Drug-Drug Interaction Data To Predict Magnitudes of Uncharacterized Interactions between Antiretroviral Drugs and Comedications
- PMID: 29686151
- PMCID: PMC6021627
- DOI: 10.1128/AAC.00717-18
Analysis of Clinical Drug-Drug Interaction Data To Predict Magnitudes of Uncharacterized Interactions between Antiretroviral Drugs and Comedications
Abstract
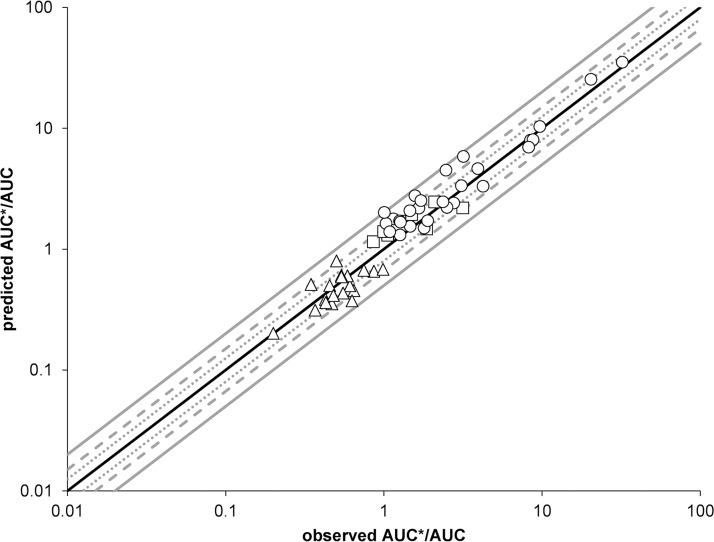
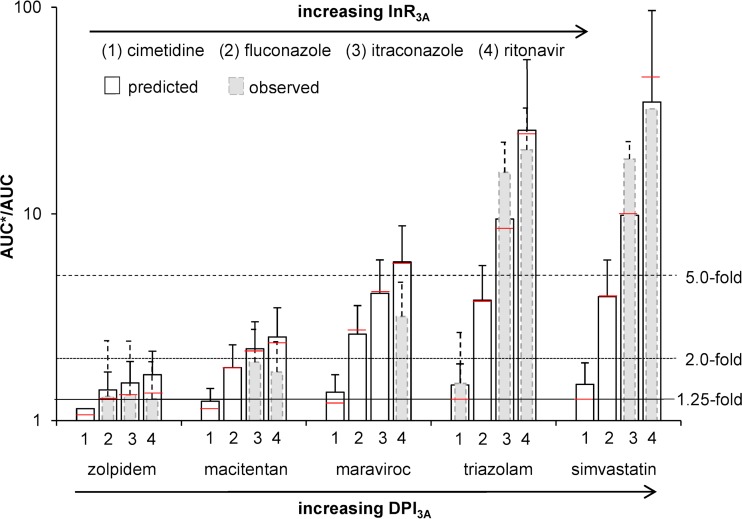
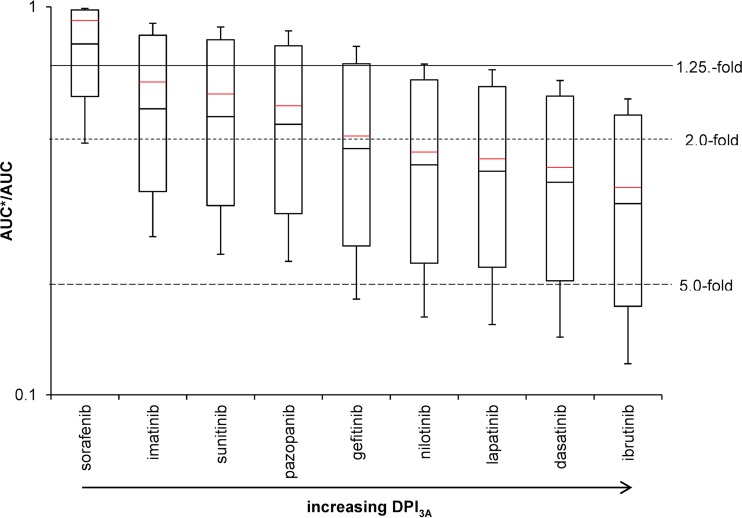
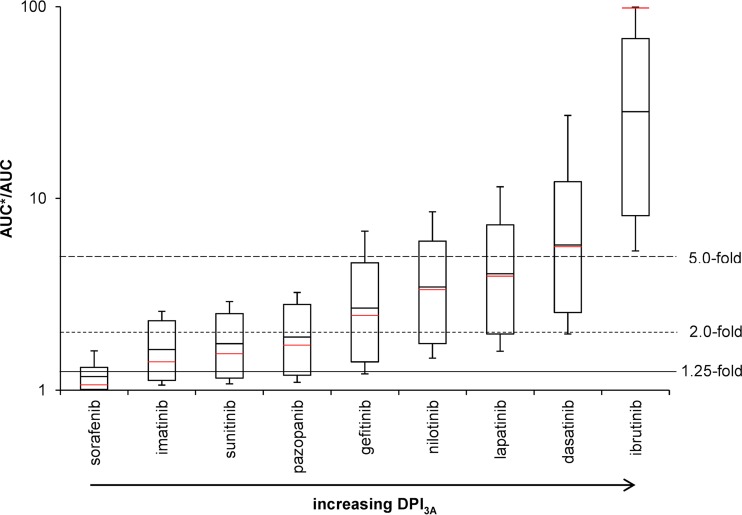
Despite their high potential for drug-drug interactions (DDI), clinical DDI studies of antiretroviral drugs (ARVs) are often lacking, because the full range of potential interactions cannot feasibly or pragmatically be studied, with some high-risk DDI studies also being ethically difficult to undertake. Thus, a robust method to screen and to predict the likelihood of DDIs is required. We developed a method to predict DDIs based on two parameters: the degree of metabolism by specific enzymes, such as CYP3A, and the strength of an inhibitor or inducer. These parameters were derived from existing studies utilizing paradigm substrates, inducers, and inhibitors of CYP3A to assess the predictive performance of this method by verifying predicted magnitudes of changes in drug exposure against clinical DDI studies involving ARVs. The derived parameters were consistent with the FDA classification of sensitive CYP3A substrates and the strength of CYP3A inhibitors and inducers. Characterized DDI magnitudes (n = 68) between ARVs and comedications were successfully quantified, meaning 53%, 85%, and 98% of the predictions were within 1.25-fold (0.80 to 1.25), 1.5-fold (0.66 to 1.48), and 2-fold (0.66 to 1.94) of the observed clinical data. In addition, the method identifies CYP3A substrates likely to be highly or, conversely, minimally impacted by CYP3A inhibitors or inducers, thus categorizing the magnitude of DDIs. The developed effective and robust method has the potential to support a more rational identification of dose adjustment to overcome DDIs, being particularly relevant in an HIV setting, given the treatment's complexity, high DDI risk, and limited guidance on the management of DDIs.
Keywords: CYP3A; HIV infection; antiretroviral drug; comedication; drug-drug interaction.
Copyright © 2018 Stader et al.
Figures


References
-
- Marzolini C, Elzi L, Gibbons S, Weber R, Fux C, Furrer H, Chave J-P, Cavassini M, Bernasconi E, Calmy A, Vernazza P, Khoo S, Ledergerber B, Back D, Battegay M. 2010. Prevalence of comedications and effect of potential drug-drug interactions in the Swiss HIV Cohort Study. Antiviral Ther 15:413. doi: 10.3851/IMP1540. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
