

Impact of enhanced recovery after surgery programs on pancreatic surgery: A meta-analysis
- PMID: 29686474
- PMCID: PMC5910550
- DOI: 10.3748/wjg.v24.i15.1666
Impact of enhanced recovery after surgery programs on pancreatic surgery: A meta-analysis
Abstract
Aim: To evaluate the impact of enhanced recovery after surgery (ERAS) programs on postoperative complications of pancreatic surgery.
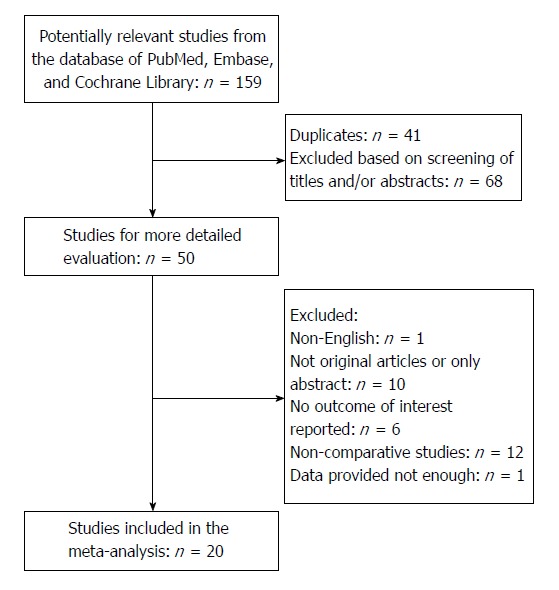
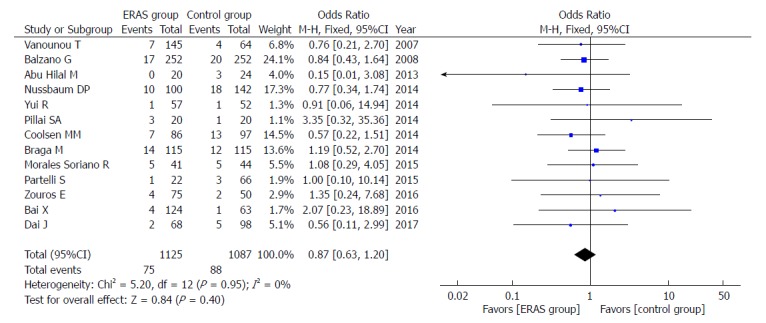
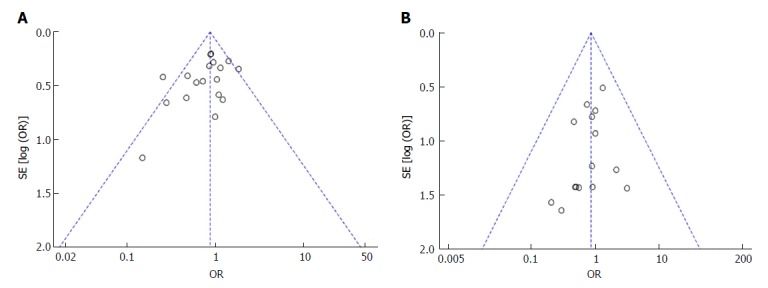
Methods: Computer searches were performed in databases (including PubMed, Cochrane Library and Embase) for randomized controlled trials or case-control studies describing ERAS programs in patients undergoing pancreatic surgery published between January 1995 and August 2017. Two researchers independently evaluated the quality of the studies' extracted data that met the inclusion criteria and performed a meta-analysis using RevMan5.3.5 software. Forest plots, demonstrating the outcomes of the ERAS group vs the control group after pancreatic surgery, and funnel plots were used to evaluate potential publication bias.
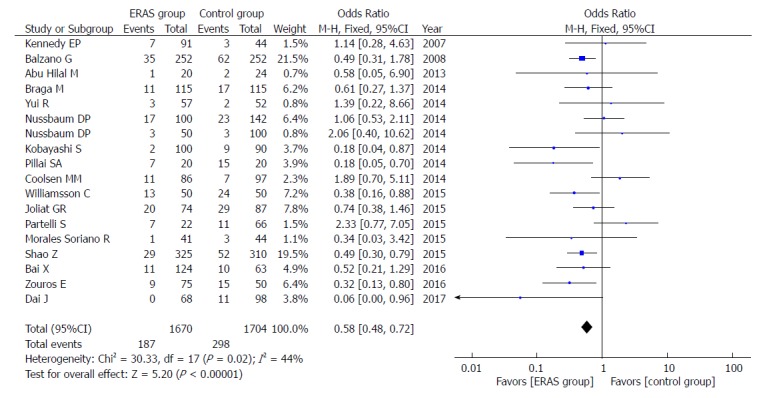
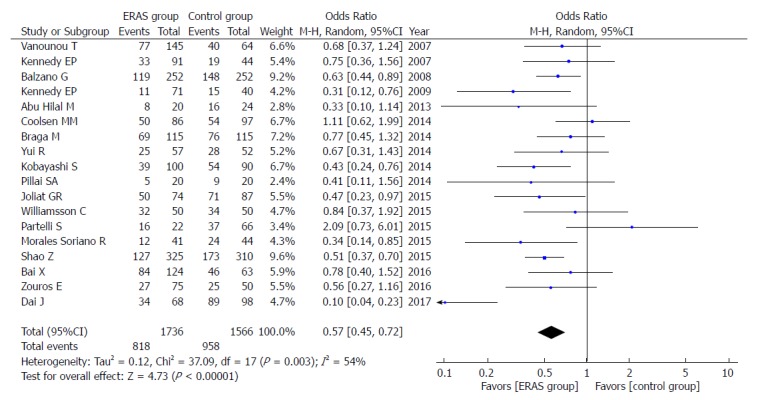
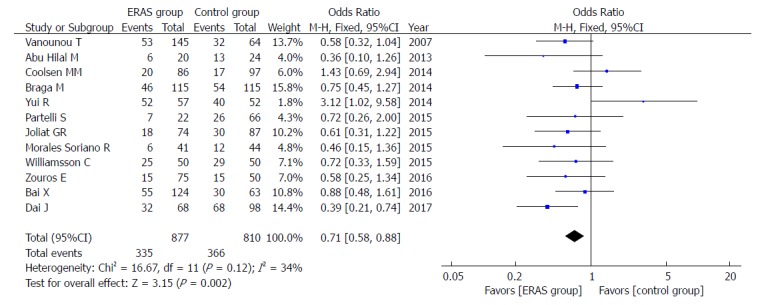
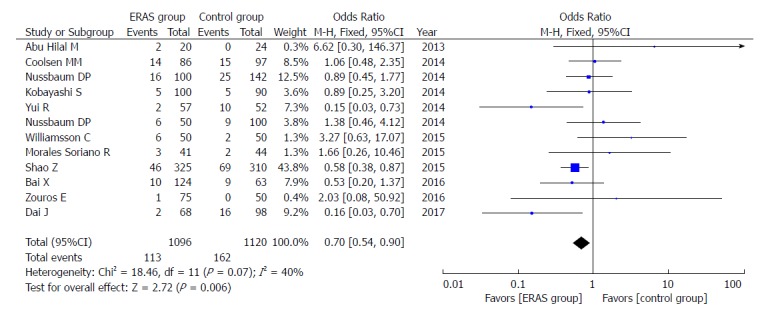
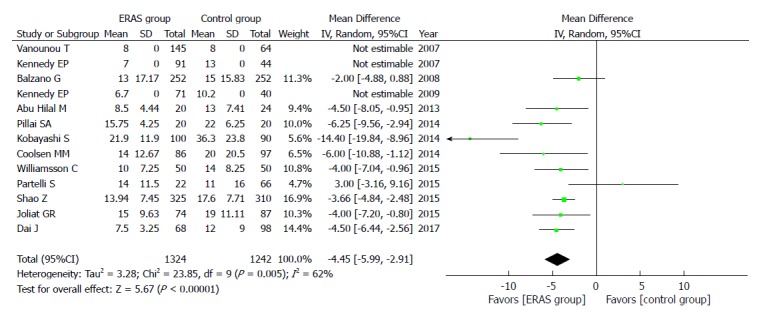
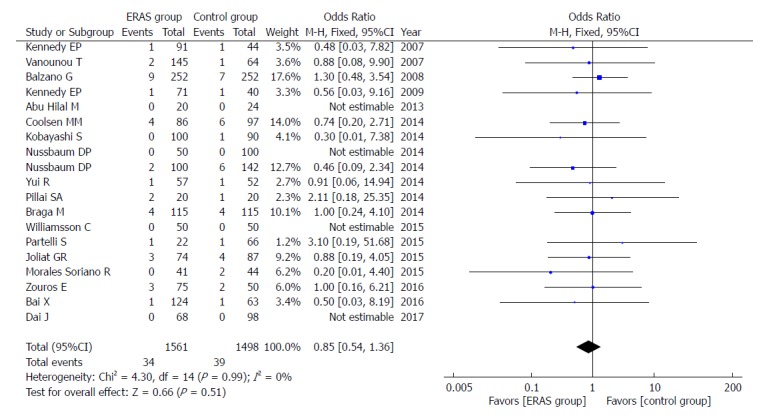
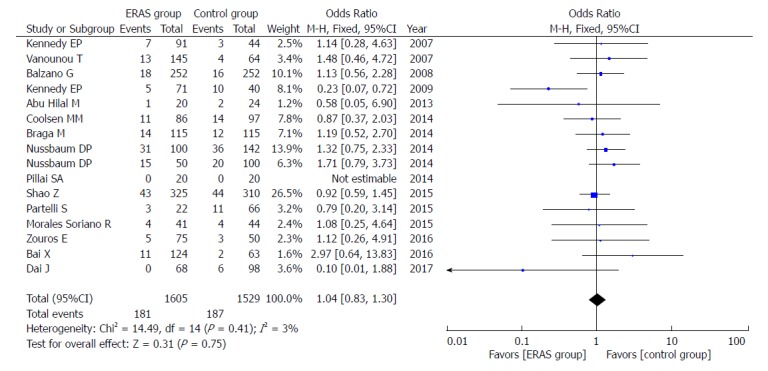
Results: Twenty case-control studies including 3694 patients, published between January 1995 and August 2017, were selected for the meta-analysis. This study included the ERAS group (n = 1886) and the control group (n = 1808), which adopted the traditional perioperative management. Compared to the control group, the ERAS group had lower delayed gastric emptying rates [odds ratio (OR) = 0.58, 95% confidence interval (CI): 0.48-0.72, P < 0.00001], lower postoperative complication rates (OR = 0.57, 95%CI: 0.45-0.72, P < 0.00001), particularly for the mild postoperative complications (Clavien-Dindo I-II) (OR = 0.71, 95%CI: 0.58-0.88, P = 0.002), lower abdominal infection rates (OR = 0.70, 95%CI: 0.54-0.90, P = 0.006), and shorter postoperative length of hospital stay (PLOS) (WMD = -4.45, 95%CI: -5.99 to -2.91, P < 0.00001). However, there were no significant differences in complications, such as, postoperative pancreatic fistulas, moderate to severe complications (Clavien-Dindo III- V), mortality, readmission and unintended reoperation, in both groups.
Conclusion: The perioperative implementation of ERAS programs in pancreatic surgery is safe and effective, can decrease postoperative complication rates, and can promote recovery for patients.
Keywords: Enhanced recovery after surgery; Meta-analysis; Pancreatic surgery; Postoperative complication.
Conflict of interest statement
Conflict-of-interest statement: The authors deny any conflict of interest.
Figures

References
-
- Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth. 1997;78:606–617. - PubMed
-
- Basse L, Raskov HH, Hjort Jakobsen D, Sonne E, Billesbølle P, Hendel HW, Rosenberg J, Kehlet H. Accelerated postoperative recovery programme after colonic resection improves physical performance, pulmonary function and body composition. Br J Surg. 2002;89:446–453. - PubMed
-
- Arsalani-Zadeh R, ElFadl D, Yassin N, MacFie J. Evidence-based review of enhancing postoperative recovery after breast surgery. Br J Surg. 2011;98:181–196. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
