

Decision uncertainty and value of further research: a case-study in fenestrated endovascular aneurysm repair for complex abdominal aortic aneurysms
- PMID: 29686541
- PMCID: PMC5902886
- DOI: 10.1186/s12962-018-0098-7
Decision uncertainty and value of further research: a case-study in fenestrated endovascular aneurysm repair for complex abdominal aortic aneurysms
Abstract
Background: Fenestrated endovascular aneurysm repair (fEVAR) is a new approach for complex abdominal aortic aneurysms, limited to a few specialist centers, with limited evidence base. We developed a cost-effectiveness decision model of fEVAR compared to open surgical repair (OSR) to investigate the likely direction of costs and benefits and inform further research projects on this technology.
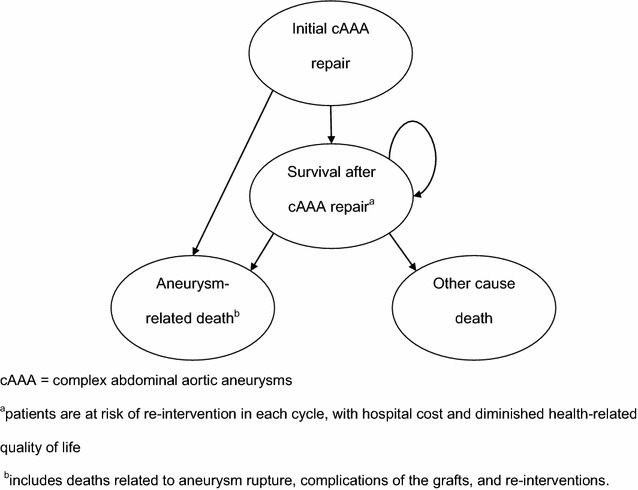
Methods: A systematic review with meta-analysis and a four-state Markov model were used to estimate the cost-effectiveness of fEVAR versus OSR. We used a recent coverage with evidence development framework to characterize the main sources of uncertainty and inform decisions about the type of further research that would be most worthwhile and feasible.
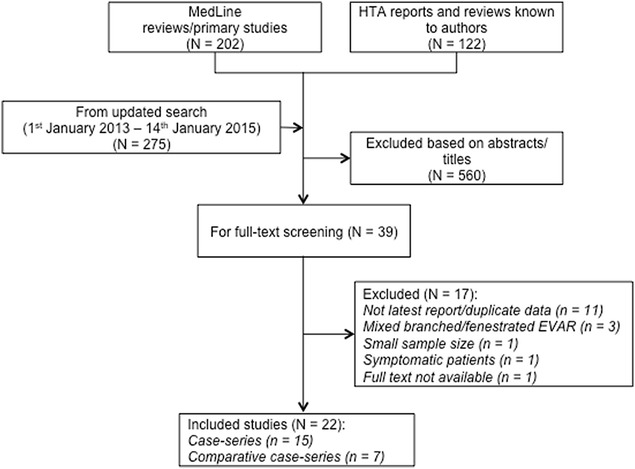
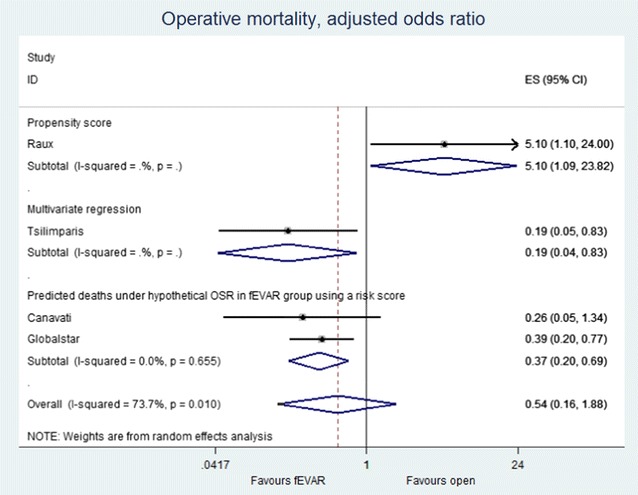
Results: Seven observational comparative studies were identified, of which four presented odds ratios adjusted for confounders. The odds ratios for operative mortality varied widely between studies. Assuming a central estimate of the odds ratio of 0.54 (95% CI 0.05-6.24), the decision model estimated that the incremental cost per quality adjusted life year (QALY) was £74,580/QALY with a probability of 9 and 16% of being cost-effective at standard cost-effectiveness thresholds of £20,000/QALY and £30,000/QALY, respectively. The Expected Value of Perfect Information over 10 years at a threshold of £20,000/QALY was £11.2 million. Operative mortality contributed to most of the uncertainty in the decision model.
Conclusions: In the case of "maturing technologies", decision modelling indicates the likely direction of costs and benefits and guides the development of further research projects. In our analysis of fEVAR versus OSR, decision uncertainty, particularly around operative mortality, might be effectively resolved by a short-term RCT, or possibly a well-conducted comparative observational study. Decision makers may consider that a conditional coverage decision is warranted with assessments required to make this type of recommendation depending on local priorities and circumstances.
Keywords: Cost-effectiveness; Coverage with evidence development; Medical devices; Value of information.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
