

How to manage various arrhythmias and sudden cardiac death in the cardiovascular intensive care
- PMID: 29686877
- PMCID: PMC5896158
- DOI: 10.1186/s40560-018-0292-x
How to manage various arrhythmias and sudden cardiac death in the cardiovascular intensive care
Erratum in
-
Correction to: How to manage various arrhythmias and sudden cardiac death in the cardiovascular intensive care.J Intensive Care. 2018 May 24;6:31. doi: 10.1186/s40560-018-0300-1. eCollection 2018. J Intensive Care. 2018. PMID: 29849434 Free PMC article.
Abstract
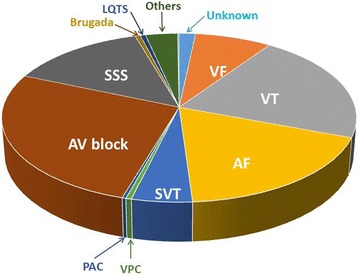
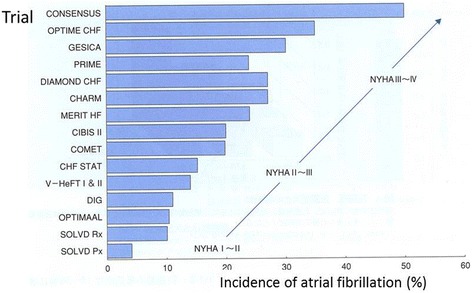
In the clinical practice of cardiovascular critical care, we often observe a variety of arrhythmias in the patients either with (secondary) or without (idiopathic) underlying heart diseases. In this manuscript, the clinical background and management of various arrhythmias treated in the CCU/ICU will be reviewed. The mechanism and background of lethal ventricular tachyarrhythmias vary as time elapses after the onset of MI that should be carefully considered to select a most suitable therapy. In the category of non-ischemic cardiomyopathy, several diseases are known to be complicated by the various ventricular tachyarrhythmias with some specific mechanisms. According to the large-scale registry data, the most common arrhythmia is atrioventricular block. It is essential for the decision of permanent pacemaker indication to rule out the presence of transient causes such as ischemia and electrolyte abnormalities. The prevalence of atrial fibrillation (AF) is very high in the patients with heart failure (HF) and myocardial infarction (MI). AF and HF have a reciprocal causal relationship; thus, both are associated with the poor prognosis. Paroxysmal AF occurs in 5 to 20% during the acute phase of MI and triggered by several specific factors including pump failure, atrial ischemia, and autonomic instability. After the total management of patients with various arrhythmias and basic heart diseases, the risk of sudden cardiac death should be stratified for each patient to assess the individual need for preventive therapies. Finally, it is recommended that the modalities of the treatment and prophylaxis should be selected on a case-by-case basis in the scene of critical care.
Keywords: Acute myocardial infarction; Arrhythmias; Cardiovascular intensive care; Congestive heart failure; Electrical storm.
Conflict of interest statement
Not applicable.Not applicable.The author declares that he has no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Ueno A, Kobayashi Y, Murata H et al The short-term prognosis of the patients with ventricular tachycardia and fibrillation: from the registry data of Tokyo CCU Network for 3 years. The proceedings of the 37th scientific meeting of Tokyo CCU Network. ICU and CCU 2018 (In press).
-
- Harris AS. Delayed development of ventricular ectopic rhythms following experimentary coronary occlusion. Circulation 1950;1:1318–1328. - PubMed
-
- Scherlag BJ, Lazzara R. In: Mandel WJ, editor. Ischemic arrhythmias: basic mechanisms. In cardiac arrhythmias. Their mechanisms, diagnosis, and management. Philaderphia: Lippincott Co; 1980. p. PP366–95.
-
- Kobayashi Y. VT/VF storm in acute myocardial infarction (In japanese). Medical Topic Sesies Huseimyaku 2017 (Edited by Sugimoto K and Inoue H). Medical Review Co. Osaka Japan, 2017. P166-175.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
