

Improved stratification of ALS clinical trials using predicted survival
- PMID: 29687024
- PMCID: PMC5899911
- DOI: 10.1002/acn3.550
Improved stratification of ALS clinical trials using predicted survival
Abstract
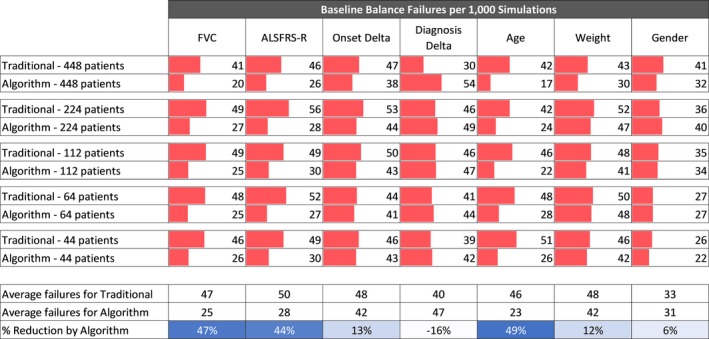
Introduction: In small trials, randomization can fail, leading to differences in patient characteristics across treatment arms, a risk that can be reduced by stratifying using key confounders. In ALS trials, riluzole use (RU) and bulbar onset (BO) have been used for stratification. We hypothesized that randomization could be improved by using a multifactorial prognostic score of predicted survival as a single stratifier.
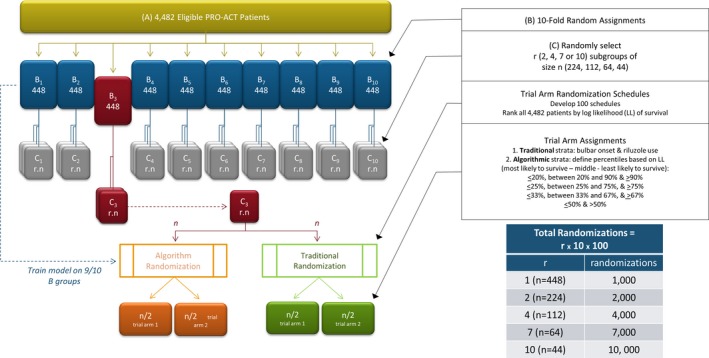
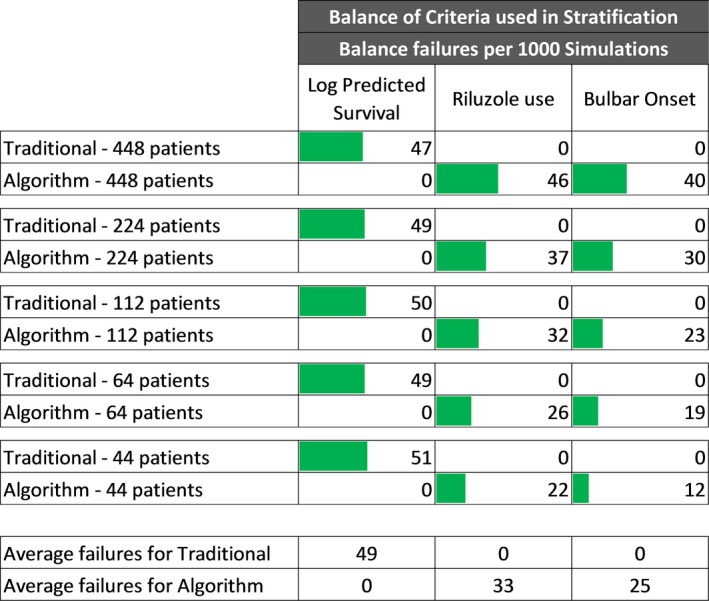
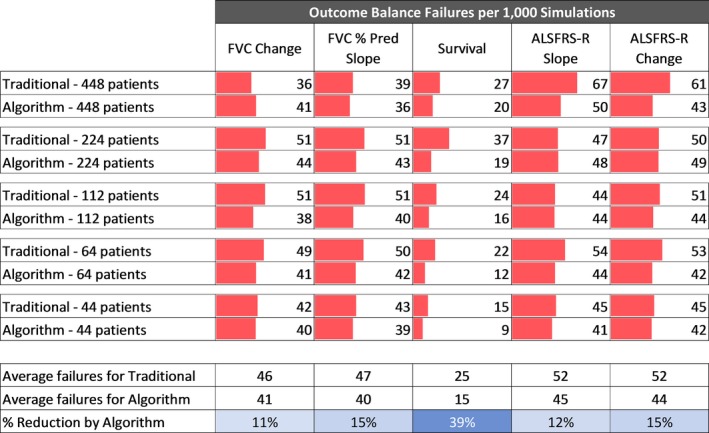
Methods: We defined a randomization failure as a significant difference between treatment arms on a characteristic. We compared randomization failure rates when stratifying for RU and BO ("traditional stratification") to failure rates when stratifying for predicted survival using a predictive algorithm. We simulated virtual trials using the PRO-ACT database without application of a treatment effect to assess balance between cohorts. We performed 100 randomizations using each stratification method - traditional and algorithmic. We applied these stratification schemes to a randomization simulation with a treatment effect using survival as the endpoint and evaluated sample size and power.
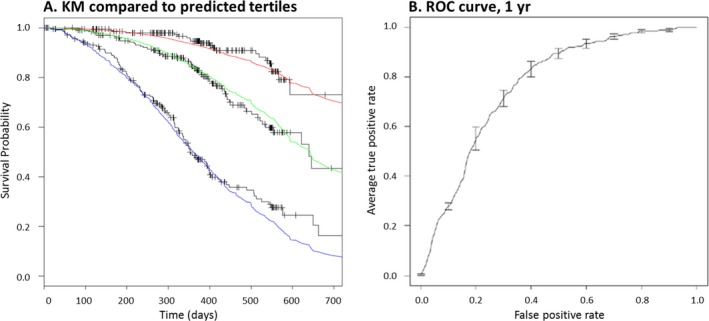
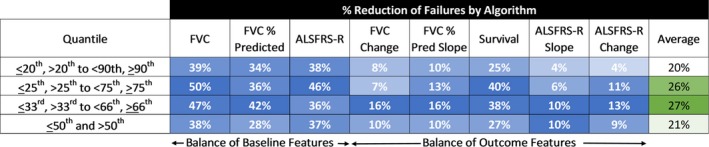
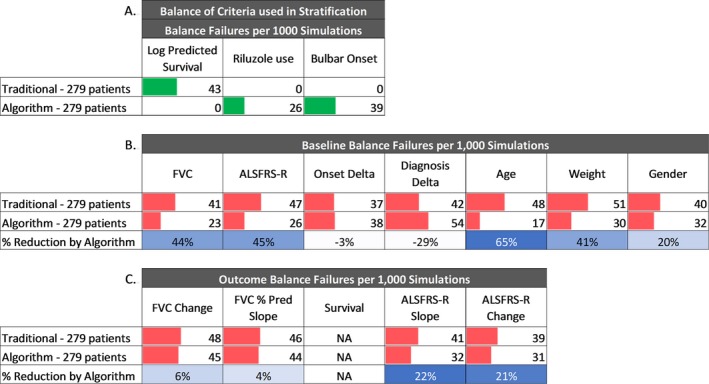
Results: Stratification by predicted survival met with fewer failures than traditional stratification. Stratifying predicted survival into tertiles performed best. Stratification by predicted survival was validated with an external dataset, the placebo arm from the BENEFIT-ALS trial. Importantly, we demonstrated a substantial decrease in sample size required to reach statistical power.
Conclusions: Stratifying randomization based on predicted survival using a machine learning algorithm is more likely to maintain balance between trial arms than traditional stratification methods. The methodology described here can translate to smaller, more efficient clinical trials for numerous neurological diseases.
Keywords: clinical trial stratification; trial methodology predictive analytics.
Figures

References
-
- Bensimon G, Lacomblez L, Meininger V. A controlled trial of riluzole in amyotrophic lateral sclerosis. ALS/Riluzole Study Group. N Engl J Med. 1994;330:585–591. - PubMed
-
- Lacomblez L, Bensimon G, Leigh PN, et al. Dose‐ranging study of riluzole in amyotrophic lateral sclerosis. Amyotrophic lateral Sclerosis/Riluzole Study Group II. Lancet 1996;347:1425–1431. - PubMed
-
- Lacomblez L, Bensimon G, Leigh PN, et al. A confirmatory dose‐ranging study of riluzole in ALS. ALS/Riluzole Study Group‐II. Neurology 1996;47(6 Suppl 4):S242–S250. - PubMed
-
- Kernan WN, Viscoli CM, Makuch RW, et al. Stratified randomization for clinical trials. J Clin Epidemiol 1999;52:19–26. - PubMed
-
- Armitage P. Fisher, Bradford Hill, and randomization. Int J Epidemiol 2003;32:925–928. https://doi.org/10.1093/ije/dyg286. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
