

Ten-year association of coronary artery calcium with atherosclerotic cardiovascular disease (ASCVD) events: the multi-ethnic study of atherosclerosis (MESA)
- PMID: 29688297
- PMCID: PMC6030975
- DOI: 10.1093/eurheartj/ehy217
Ten-year association of coronary artery calcium with atherosclerotic cardiovascular disease (ASCVD) events: the multi-ethnic study of atherosclerosis (MESA)
Abstract
Aims: While coronary artery calcium (CAC) has been extensively validated for predicting clinical events, most outcome studies of CAC have evaluated coronary heart disease (CHD) rather than atherosclerotic cardiovascular disease (ASCVD) events (including stroke). Also, virtually all CAC studies are of short- or intermediate-term follow-up, so studies across multi-ethnic cohorts with long-term follow-up are warranted prior to widespread clinical use. We sought to evaluate the contribution of CAC using the population-based MESA cohort with over 10 years of follow-up for ASCVD events, and whether the association of CAC with events varied by sex, race/ethnicity, or age category.
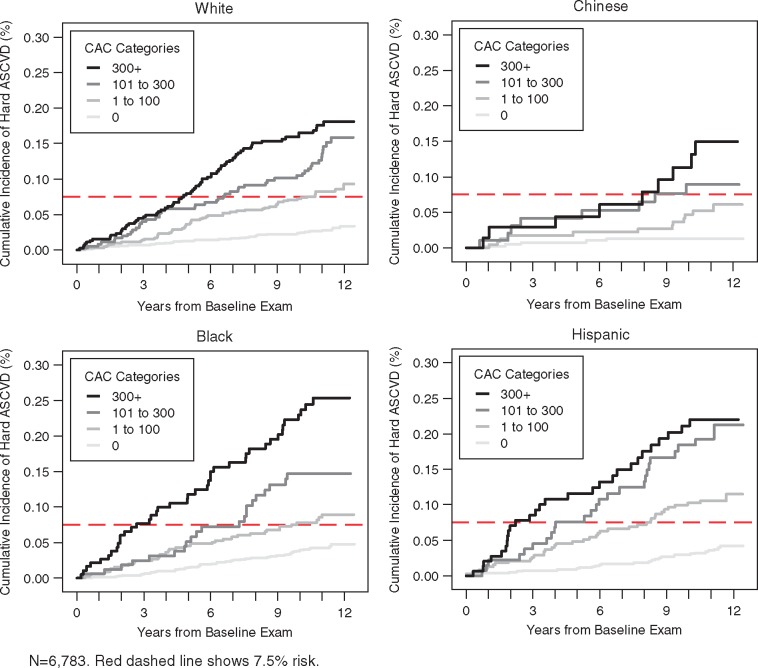
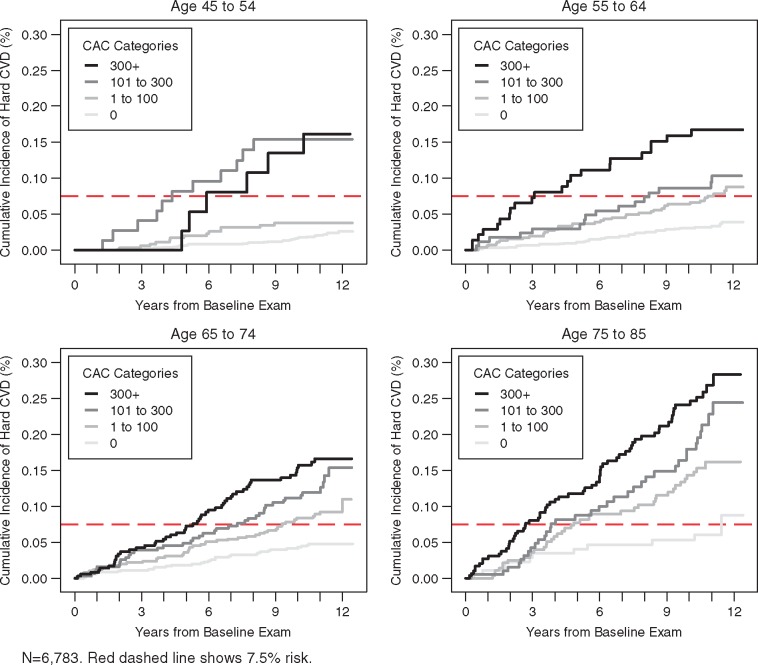
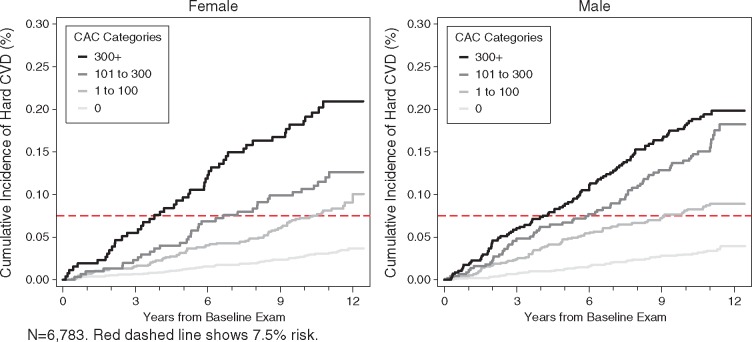
Methods and results: We utilized MESA, a prospective multi-ethnic cohort study of 6814 participants (51% women), aged 45-84 years, free of clinical CVD at baseline. We evaluated the relationship between CAC and incident ASCVD using Cox regression models adjusted for age, race/ethnicity, sex, education, income, cigarette smoking status, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, diabetes, lipid-lowering medication, systolic blood pressure, antihypertensive medication, intentional physical exercise, and body mass index. Only the first event for each individual was used in the analysis. Overall, 500 incident ASCVD (7.4%) events were observed in the total study population over a median of 11.1 years. Hard ASCVD included 217 myocardial infarction, 188 strokes (not transient ischaemic attack), 13 resuscitated cardiac arrest, and 82 CHD deaths. Event rates in those with CAC = 0 Agatston units ranged from 1.3% to 5.6%, while for those with CAC > 300, the 10-year event rates ranged from 13.1% to 25.6% across different age, gender, and racial subgroups. At 10 years of follow-up, all participants with CAC > 100 were estimated to have >7.5% risk regardless of demographic subset. Ten-year ASCVD event rates increased steadily across CAC categories regardless of age, sex, or race/ethnicity. For each doubling of CAC, we estimated a 14% relative increment in ASCVD risk, holding all other risk factors constant. This association was not significantly modified by age, sex, race/ethnicity, or baseline lipid-lowering use.
Conclusions: Coronary artery calcium is associated strongly and in a graded fashion with 10-year risk of incident ASCVD as it is for CHD, independent of standard risk factors, and similarly by age, gender, and ethnicity. While 10-year event rates in those with CAC = 0 were almost exclusively below 5%, those with CAC ≥ 100 were consistently above 7.5%, making these potentially valuable cutpoints for the consideration of preventive therapies. Coronary artery calcium strongly predicts risk with the same magnitude of effect in all races, age groups, and both sexes, which makes it among the most useful markers for predicting ASCVD risk.
Figures
Comment in
-
Is it time to move from treating risk factors of the disease to treating the disease?Eur Heart J. 2018 Jul 1;39(25):2409-2411. doi: 10.1093/eurheartj/ehy343. Eur Heart J. 2018. PMID: 29982444 No abstract available.
References
-
- Goff DC Jr, Lloyd-Jones DM, Bennett G, Coady S, D'Agostino RB Sr, Gibbons R, Greenland P, Lackland DT, Levy D, O’Donnell CJ, Robinson JG, Schwartz JS, Shero ST, Smith SC Jr, Sorlie P, Stone NJ, Wilson PW; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;63:2935–2959. - PMC - PubMed
-
- Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, Goldberg AC, Gordon D, Levy D, Lloyd-Jones DM, McBride P, Schwartz JS, Shero ST, Smith SC Jr, Watson K, Wilson PW; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;63:2889–2934. - PubMed
-
- Lackland DT, Elkind MS, D’Agostino R Sr, Dhamoon MS, Goff DC Jr, Higashida RT, McClure LA, Mitchell PH, Sacco RL, Sila CA, Smith SC Jr, Tanne D, Tirschwell DL, Touzé E, Wechsler LR.. Inclusion of stroke in cardiovascular risk prediction instruments: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2012;43:1998–2027. - PubMed
-
- Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, Cooney MT, Corrà U, Cosyns B, Deaton C, Graham I, Hall MS, Hobbs FD, Løchen ML, Löllgen H, Marques-Vidal P, Perk J, Prescott E, Redon J, Richter DJ, Sattar N, Smulders Y, Tiberi M, van der Worp HB, van Dis I, Verschuren WM.. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J 2016;37:2315–2381. - PMC - PubMed
-
- Budoff MJ, Möhlenkamp S, McClelland R, Delaney JA, Bauer M, Jöckel HK, Kälsch H, Kronmal R, Nasir K, Lehmann N, Moebus S, Mukamal K, Erbel R.. A comparison of outcomes with coronary artery calcium scanning in unselected populations: the Multi-Ethnic Study of Atherosclerosis (MESA) and Heinz Nixdorf RECALL study (HNR). J Cardiovasc Comput Tomogr 2013;7:182–191. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- N01 HC095161/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- R01 HL071739/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
