

Electrocardiographic characteristics, anthropometric features, and cardiovascular risk factors in a large cohort of adolescents
- PMID: 29688314
- PMCID: PMC6212775
- DOI: 10.1093/europace/euy073
Electrocardiographic characteristics, anthropometric features, and cardiovascular risk factors in a large cohort of adolescents
Abstract
Aims: The characteristics of electrocardiographic (ECG) patterns in the general population of adolescents are insufficiently defined. The purpose of this study is to report ECG patterns and their association with anthropometric characteristics.
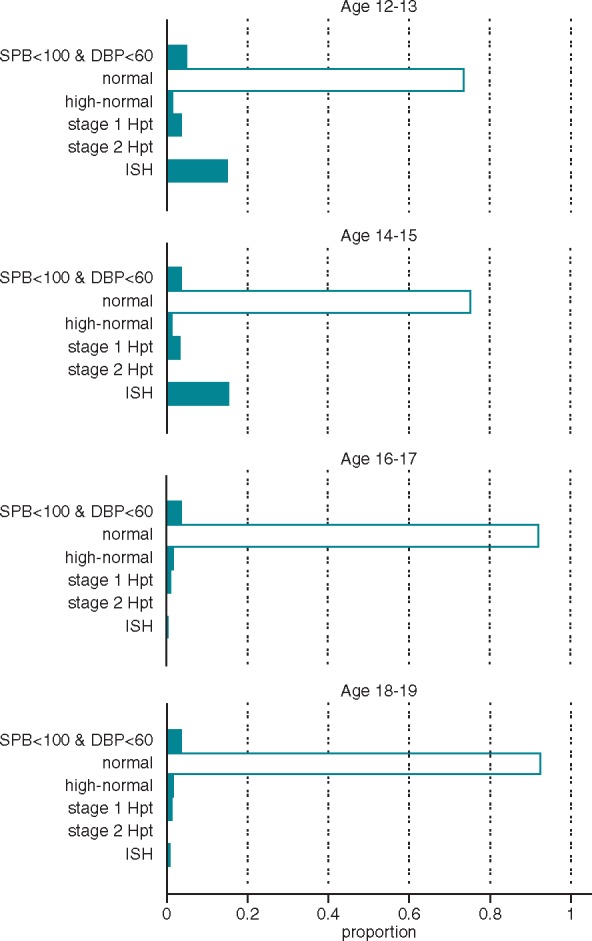
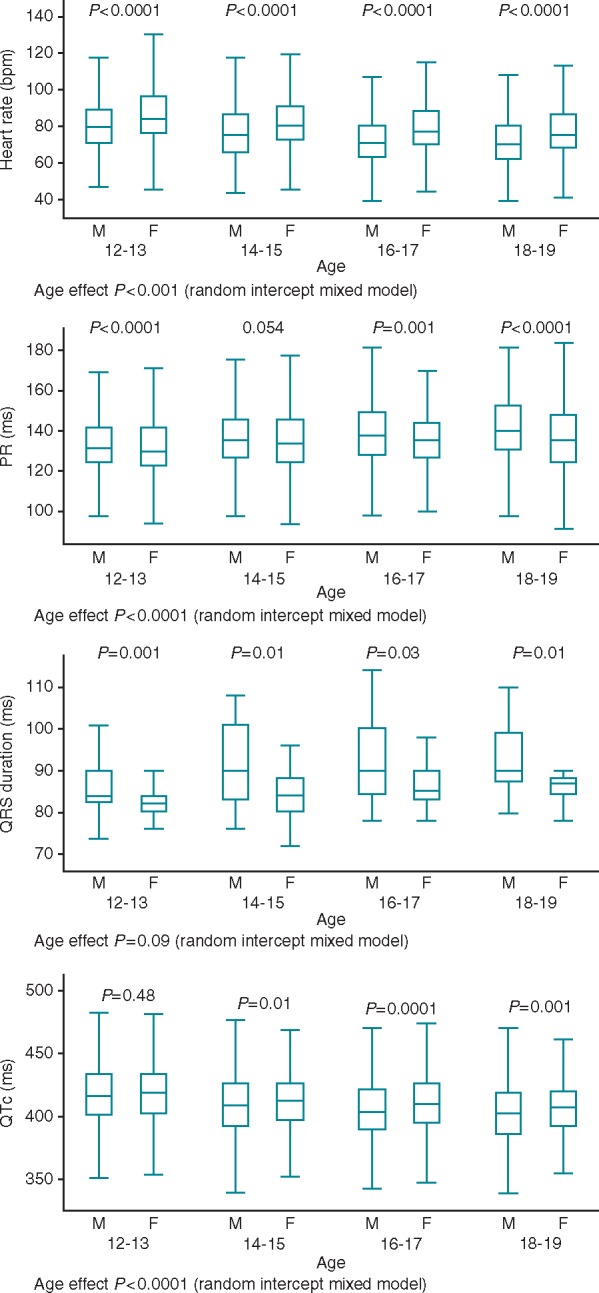
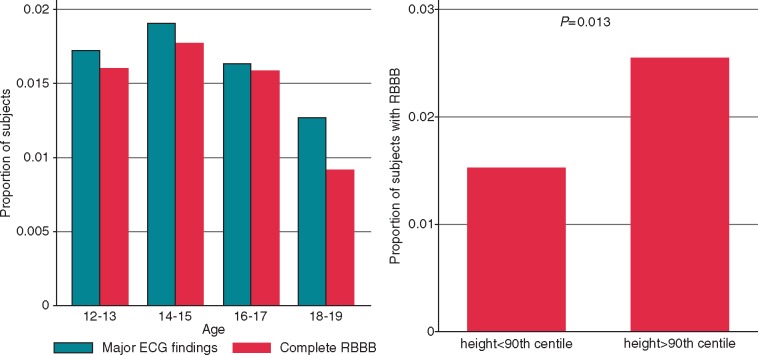
Methods and results: Twenty-four thousand and sixty-two students of Roman schools, aged 12-19, were screened with ECG and physical examinations. Electrocardiographic abnormalities were classified as either minor/non-clinically relevant or major, and anthropometric measures were evaluated per age class. Obesity prevalence was 20.9%, with a higher rate in younger students (P < 0.008 for all comparisons, except for the pair 16-17 vs. 18-19 years). Stage 1 hypertension was found in 3.14% of adolescents, Stage 2 hypertension in 0.45% of adolescents, and isolated systolic hypertension in 11.7% of adolescents. Heart rate and QT interval corrected for heart rate (QTc) decreased with increasing age. The QTc was longer in females than in males over 14 years. A higher rate of incomplete right bundle branch block (RBBB) was observed in underweight students (21.58% vs. 15.10% in non-underweight students, P < 0.0001). Complete RBBB was the most common major ECG abnormality (1.6%). It was associated with height irrespective of age, sex, and body mass index (odds ratio 17.9; 95% confidence interval 5.0-64.6) and more frequent in students regularly practicing physical activity (1.80% vs. 1.02%, P = 0.0009).
Conclusion: Heart rate and QTc decreased with increasing age. The QTc was longer in females than in males over 14 years. RBBB was the most common major abnormality and was associated with higher stature. The prevalence of some cardiovascular risk factors in adolescents is provided.
Figures
Similar articles
-
Anthropometric screening for silent cardiovascular risk factors in adolescents: The PEP Family Heart Study.Atherosclerosis. 2010 Aug;211(2):667-71. doi: 10.1016/j.atherosclerosis.2010.03.032. Epub 2010 Apr 4. Atherosclerosis. 2010. PMID: 20417933
-
Prevalence of abnormal electrocardiograms in a large, unselected population undergoing pre-participation cardiovascular screening.Eur Heart J. 2007 Aug;28(16):2006-10. doi: 10.1093/eurheartj/ehm219. Epub 2007 Jul 10. Eur Heart J. 2007. PMID: 17623682
-
Relationship of QT interval duration with carotid intima media thickness in a clinically healthy population undergoing cardiovascular risk screening.J Intern Med. 2005 Mar;257(3):238-46. doi: 10.1111/j.1365-2796.2004.01436.x. J Intern Med. 2005. PMID: 15715680
-
Electrocardiographic changes in centenarians: a study on 42 subjects and comparison with the literature.Gerontology. 2012;58(3):216-20. doi: 10.1159/000330801. Epub 2011 Sep 7. Gerontology. 2012. PMID: 21912098 Review.
-
Electrocardiographic right and left bundle branch block patterns in athletes: prevalence, pathology, and clinical significance.J Electrocardiol. 2015 May-Jun;48(3):380-4. doi: 10.1016/j.jelectrocard.2015.03.015. Epub 2015 Mar 14. J Electrocardiol. 2015. PMID: 25836379 Review.
Cited by
-
Electrocardiographic characteristics of pediatric and adolescent football players.Sports Med Health Sci. 2023 Dec 15;6(2):179-184. doi: 10.1016/j.smhs.2023.12.004. eCollection 2024 Jun. Sports Med Health Sci. 2023. PMID: 38708327 Free PMC article.
-
QTc dispersion and interval changes in drug-free borderline personality disorder adolescents.Eur Child Adolesc Psychiatry. 2020 Feb;29(2):199-203. doi: 10.1007/s00787-019-01343-3. Epub 2019 May 14. Eur Child Adolesc Psychiatry. 2020. PMID: 31089814
-
Electrocardiogram screening for school children: a cross-sectional, population-based study.Ann Saudi Med. 2025 Mar-Apr;45(2):69-78. doi: 10.5144/0256-4947.2025.69. Epub 2025 Apr 3. Ann Saudi Med. 2025. PMID: 40189851 Free PMC article.
-
Age-Related Electrocardiographic Characteristics of Male Junior Soccer Athletes.Front Cardiovasc Med. 2022 Feb 3;8:784170. doi: 10.3389/fcvm.2021.784170. eCollection 2021. Front Cardiovasc Med. 2022. PMID: 35187105 Free PMC article.
-
Comparison of Machine Learning Algorithms Using Manual/Automated Features on 12-Lead Signal Electrocardiogram Classification: A Large Cohort Study on Students Aged Between 6 to 18 Years Old.Cardiovasc Eng Technol. 2023 Dec;14(6):786-800. doi: 10.1007/s13239-023-00687-x. Epub 2023 Oct 17. Cardiovasc Eng Technol. 2023. PMID: 37848737
References
-
- Maron BJ, Friedman RA, Kligfield P, Levine BD, Viskin S, Chaitman BR. et al. Assessment of the 12-lead electrocardiogram as a screening test for detection of cardiovascular disease in healthy general populations of young people (12-25 years of age): a scientific statement from the American Heart Association and the American College of Cardiology. J Am Coll Cardiol 2014;64:1479–514. - PubMed
-
- Gulizia MM, Casolo G, Zuin G, Morichelli L, Calcagnini G, Ventimiglia V. et al. ANMCO/AIIC/SIT Consensus Information Document: definition, precision, and suitability of electrocardiographic signals of electrocardiographs, ergometry, Holter electrocardiogram, telemetry, and bedside monitoring systems. Eur Heart J Suppl 2017;19:D190–211. - PMC - PubMed
-
- Surawicz B, Childers R, Deal BJ, Gettes LS, Bailey JJ, Gorgels A. et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part III: intraventricular conduction disturbances: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Endorsed by the International Society for Computerized Electrocardiology. J Am Coll Cardiol 2009;53:976–81. - PubMed
-
- Sharma S, Drezner JA, Baggish A, Papadakis M, Wilson MG, Prutkin JM. et al. International recommendations for electrocardiographic interpretation in athletes. J Am Coll Cardiol 2017;69:1057–75. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
