

Greater fluid overload and lower interdialytic weight gain are independently associated with mortality in a large international hemodialysis population
- PMID: 29688512
- PMCID: PMC6168737
- DOI: 10.1093/ndt/gfy083
Greater fluid overload and lower interdialytic weight gain are independently associated with mortality in a large international hemodialysis population
Abstract
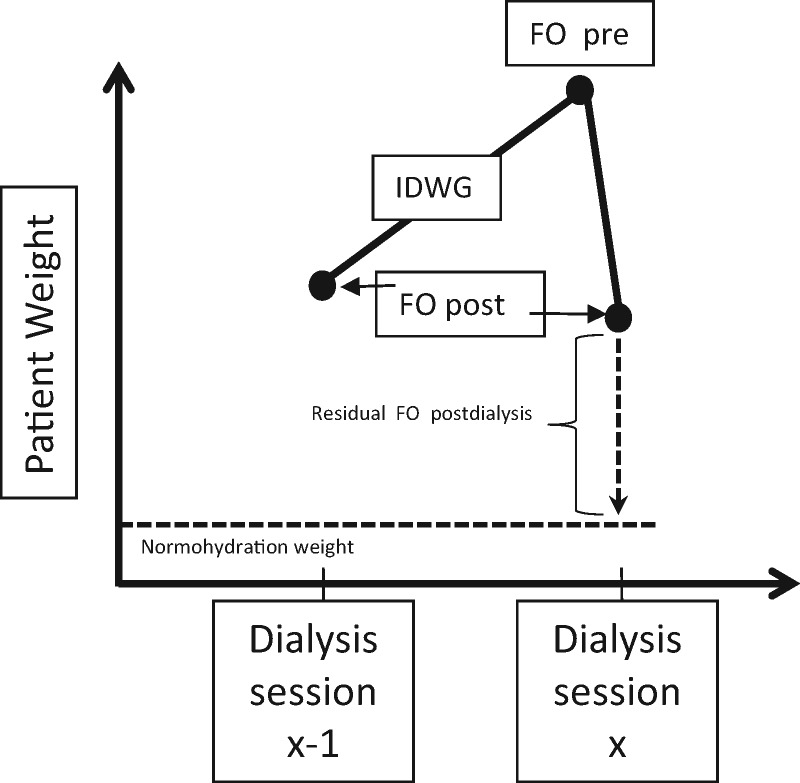
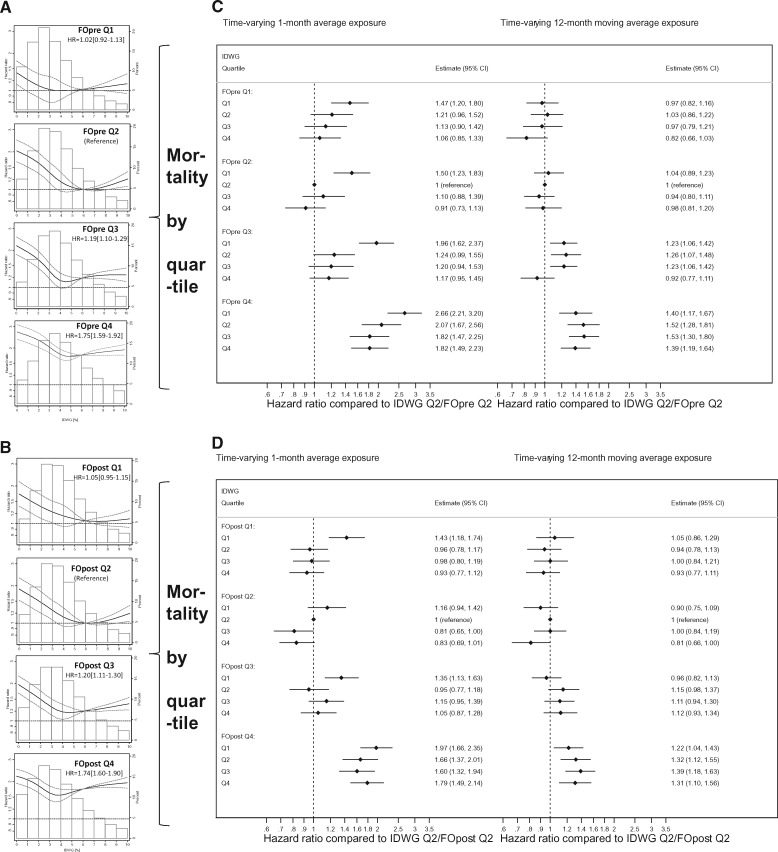
Background: Fluid overload and interdialytic weight gain (IDWG) are discrete components of the dynamic fluid balance in haemodialysis patients. We aimed to disentangle their relationship, and the prognostic importance of two clinically distinct, bioimpedance spectroscopy (BIS)-derived measures, pre-dialysis and post-dialysis fluid overload (FOpre and FOpost) versus IDWG.
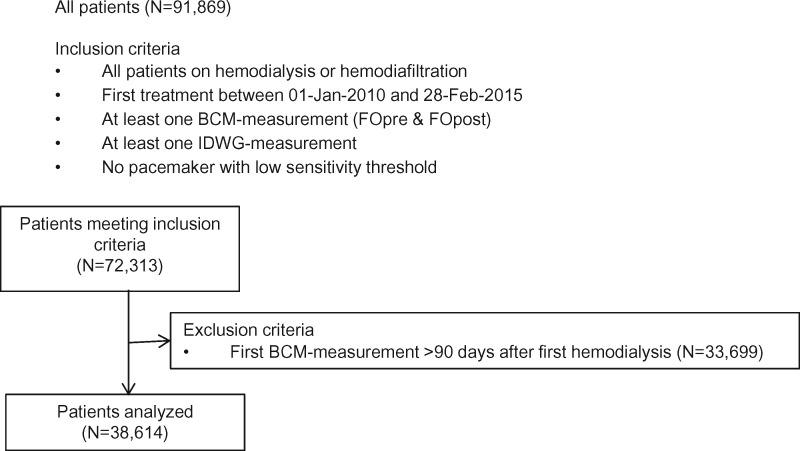
Methods: We conducted a retrospective cohort study on 38 614 incident patients with one or more BIS measurement within 90 days of haemodialysis initiation (1 October 2010 through 28 February 2015). We used fractional polynomial regression to determine the association pattern between FOpre, FOpost and IDWG, and multivariate adjusted Cox models with FO and/or IDWG as longitudinal and time-varying predictors to determine all-cause mortality risk.
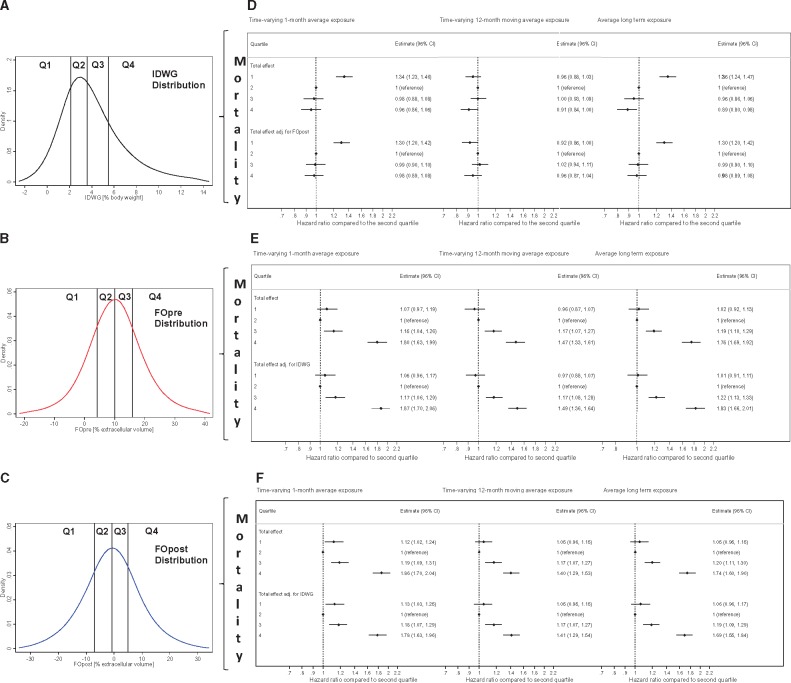
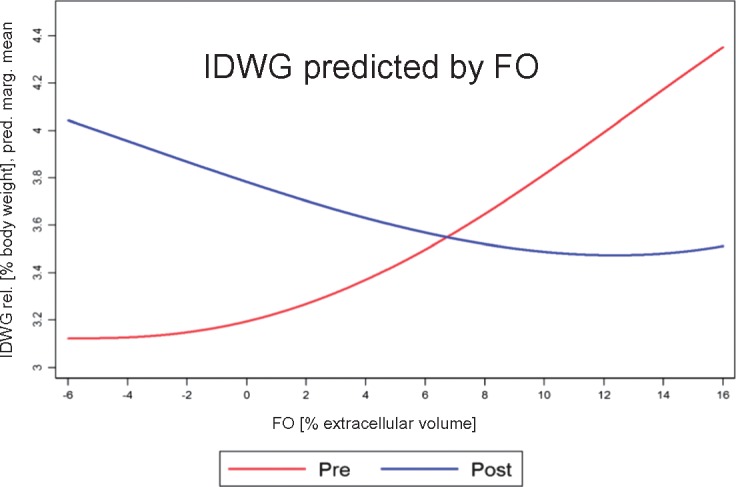
Results: In analyses using 1-month averages, patients in quartiles 3 and 4 (Q3 and Q4) of FO had an incrementally higher adjusted mortality risk compared with reference Q2, and patients in Q1 of IDWG had higher adjusted mortality compared with Q2. The highest adjusted mortality risk was observed for patients in Q4 of FOpre combined with Q1 of IDWG [hazard ratio (HR) = 2.66 (95% confidence interval 2.21-3.20), compared with FOpre-Q2/IDWG-Q2 (reference)]. Using longitudinal means of FO and IDWG only slightly altered all HRs. IDWG associated positively with FOpre, but negatively with FOpost, suggesting a link with post-dialysis extracellular volume depletion.
Conclusions: FOpre and FOpost were consistently positive risk factors for mortality. Low IDWG was associated with short-term mortality, suggesting perhaps an effect of protein-energy wasting. FOpost reflected the volume status without IDWG, which implies that this fluid marker is clinically most intuitive and may be best suited to guide volume management in haemodialysis patients.
Figures
References
-
- Ortiz A, Covic A, Fliser D. et al. Epidemiology, contributors to, and clinical trials of mortality risk in chronic kidney failure. Lancet 2014; 383: 1831–1843 - PubMed
-
- Kendrick J, Chonchol MB.. Nontraditional risk factors for cardiovascular disease in patients with chronic kidney disease. Nat Clin Pract Nephrol 2008; 4: 672–681 - PubMed
-
- Chamney PW, Wabel P, Moissl UM. et al. A whole-body model to distinguish excess fluid from the hydration of major body tissues. Am J Clin Nutr 2007; 85: 80–89 - PubMed
-
- Chazot C, Wabel P, Chamney P. et al. Importance of normohydration for the long-term survival of haemodialysis patients. Nephrol Dial Transplant 2012; 27: 2404–2410 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
