

High-resolution 3 T magnetic resonance findings in cochlear hypoplasias and incomplete partition anomalies: a pictorial essay
- PMID: 29688748
- PMCID: PMC6223158
- DOI: 10.1259/bjr.20180120
High-resolution 3 T magnetic resonance findings in cochlear hypoplasias and incomplete partition anomalies: a pictorial essay
Abstract
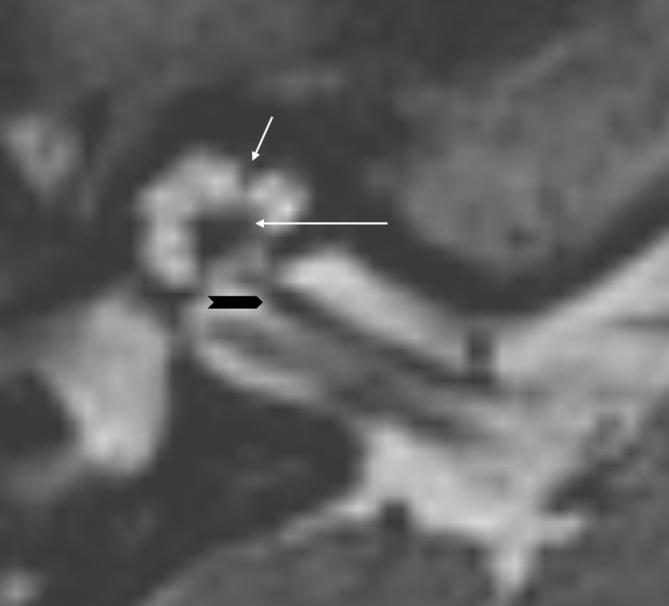
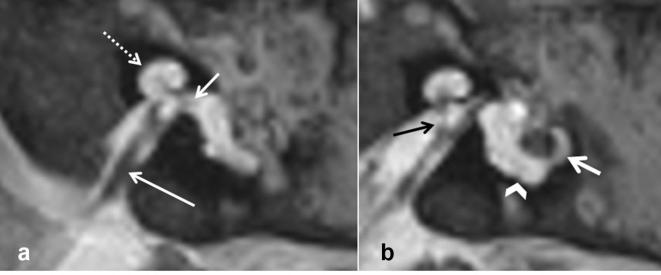
Inner ear malformations are recognized by imaging in about 20% of children with congenital sensorineural hearing loss. Normal development of the inner ear structures can be affected by many factors, including genetic anomalies as well as environmental destructive causes (ischemic, infectious, radiation and more). Recently, histopathological studies have provided new insights on the anatomy and pathogenesis of inner ear malformations, especially regarding incomplete partition and cochlear hypoplasia (CH), for which different subtypes have been identified. Factors known for interfering with normal inner ear development are numerous and sometimes act simultaneously, making the understanding of their pathophysiology more challenging. Vascular supply from the internal auditory canal seems to be critical for normal development of internal structures of the labyrinth while a premature arrest in the spatial development of the cochlea due to genetic or toxic factors may result in short cochlea (i.e.: CH). The aim of this essay is to show 3 T MRI appearances of the different subtypes of CH and incomplete partition introduced in the new classification (findings summary in Table 1).
Figures








References
-
- Nikolopoulos TP, O'Donoghue GM, Robinson KL, Holland IM, Ludman C, Gibbin KP. Preoperative radiologic evaluation in cochlear implantation. Am J Otol 1997; 18(6 Suppl): S73–4. - PubMed
-
- Dahmani-Causse M, Marx M, Deguine O, Fraysse B, Lepage B, Escudé B. Morphologic examination of the temporal bone by cone beam computed tomography: comparison with multislice helical computed tomography. Eur Ann Otorhinolaryngol Head Neck Dis 2011; 128: 230–5. doi: 10.1016/j.anorl.2011.02.016 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
