

Beyond syndromic management: Opportunities for diagnosis-based treatment of sexually transmitted infections in low- and middle-income countries
- PMID: 29689080
- PMCID: PMC5918163
- DOI: 10.1371/journal.pone.0196209
Beyond syndromic management: Opportunities for diagnosis-based treatment of sexually transmitted infections in low- and middle-income countries
Abstract
Introduction: In light of the limited impact the syndromic management approach has had on the global sexually transmitted infection (STI) epidemic, we assessed a care model comprising point-of-care (POC) STI testing, immediate treatment, and expedited partner therapy (EPT) among a cohort of young women at high HIV risk in South Africa.
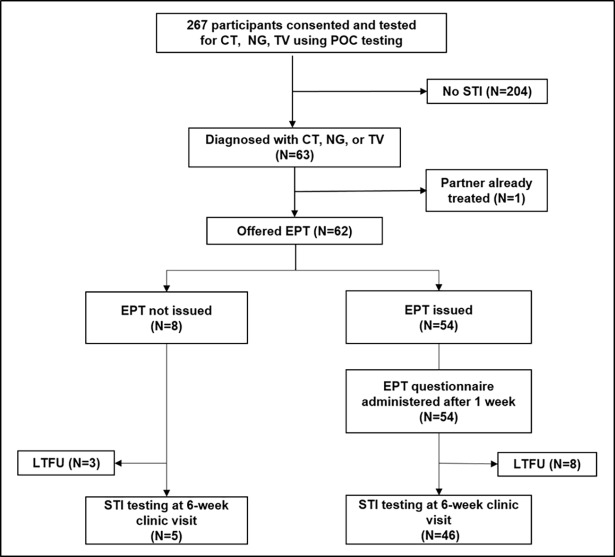
Methods and findings: HIV negative women presenting for STI care underwent POC testing for Chlamydia trachomatis (CT), Neisseria gonorrhoeae (NG) and Trichomonas vaginalis (TV), and swabs were sent for NG culture and susceptibility testing. Results were available within 2 hours and women with STIs were immediately treated and offered EPT packs, including medication, condoms, and information for sexual partners. An EPT questionnaire was administered after one week, and women retested for STIs after 6 and 12 weeks. 267 women, median age 23 (IQR 21-26), were recruited and 88.4% (236/267) reported genital symptoms. STI prevalence was CT 18.4% (95%CI 13.7-23.0), NG 5.2% (95%CI 2.6-7.9) and TV 3.0% (95%CI 1.0-5.0). After 12 weeks, all but one NG and two CT infections were cleared. No cephalosporin-resistant NG was detected. Of 63/267 women (23.6%) diagnosed with STIs, 98.4% (62/63) were offered and 87.1% (54/62) accepted EPT. At one week 88.9% (48/54) stated that their partner had taken the medication. No allergic reactions or social harms were reported. Of 51 women completing 6-week follow up, detection rates were lower amongst women receiving EPT (2.2%, 1/46) compared to those who did not (40.0%, 2/5), p = 0.023. During focus group discussions women supported the care model, because they received a rapid, specific diagnosis, and could facilitate their partners' treatment.
Conclusions: POC STI testing and EPT were acceptable to young South African women and their partners, and could play an important role in reducing STI reinfection rates and HIV risk. Larger studies should evaluate the feasibility and cost-effectiveness of implementing this strategy at population level.
Conflict of interest statement
Figures
Similar articles
-
Impact of Point-of-Care Testing on the Management of Sexually Transmitted Infections in South Africa: Evidence from the HVTN702 Human Immunodeficiency Virus Vaccine Trial.Clin Infect Dis. 2023 Mar 4;76(5):881-889. doi: 10.1093/cid/ciac824. Clin Infect Dis. 2023. PMID: 36250382 Free PMC article. Clinical Trial.
-
Attitudes of women participating in a clinical trial on point-of-care testing and home testing for STIs.Int J STD AIDS. 2020 Dec;31(14):1352-1358. doi: 10.1177/0956462420955067. Epub 2020 Sep 30. Int J STD AIDS. 2020. PMID: 32996866
-
Evaluating the utility of syndromic case management for three sexually transmitted infections in women visiting hospitals in Delhi, India.Sci Rep. 2017 May 3;7(1):1465. doi: 10.1038/s41598-017-01422-y. Sci Rep. 2017. PMID: 28469158 Free PMC article.
-
Diagnosis and Treatment of Sexually Transmitted Infections: A Review.JAMA. 2022 Jan 11;327(2):161-172. doi: 10.1001/jama.2021.23487. JAMA. 2022. PMID: 35015033 Review.
-
Diagnosing sexually transmitted infections in resource-constrained settings: challenges and ways forward.J Int AIDS Soc. 2019 Aug;22 Suppl 6(Suppl Suppl 6):e25343. doi: 10.1002/jia2.25343. J Int AIDS Soc. 2019. PMID: 31468679 Free PMC article.
Cited by
-
Assessment of Antibiotic Resistance and Efflux Pump Gene Expression in Neisseria Gonorrhoeae Isolates from South Africa by Quantitative Real-Time PCR and Regression Analysis.Int J Microbiol. 2022 Oct 21;2022:7318325. doi: 10.1155/2022/7318325. eCollection 2022. Int J Microbiol. 2022. PMID: 36312786 Free PMC article.
-
Recent advances in the epidemiology, diagnosis, and management of Trichomonas vaginalis infection.F1000Res. 2019 Sep 20;8:F1000 Faculty Rev-1666. doi: 10.12688/f1000research.19972.1. eCollection 2019. F1000Res. 2019. PMID: 31583080 Free PMC article. Review.
-
A high burden of asymptomatic genital tract infections undermines the syndromic management approach among adolescents and young adults in South Africa: implications for HIV prevention efforts.BMC Infect Dis. 2018 Oct 3;18(1):499. doi: 10.1186/s12879-018-3380-6. BMC Infect Dis. 2018. PMID: 30285705 Free PMC article.
-
Prevalence of yaws and syphilis in the Ashanti region of Ghana and occurrence of H. ducreyi, herpes simplex virus 1 and herpes simplex virus 2 in skin lesions associated with treponematoses.PLoS One. 2024 May 22;19(5):e0295088. doi: 10.1371/journal.pone.0295088. eCollection 2024. PLoS One. 2024. PMID: 38776332 Free PMC article.
-
Sexually transmitted infections among women randomised to depot medroxyprogesterone acetate, a copper intrauterine device or a levonorgestrel implant.Sex Transm Infect. 2021 Jun;97(4):249-255. doi: 10.1136/sextrans-2020-054590. Epub 2020 Nov 18. Sex Transm Infect. 2021. PMID: 33208512 Free PMC article. Clinical Trial.
References
-
- UNAIDS (2016) AIDS by the numbers. Available from: http://www.unaids.org/en/resources/documents/2016/AIDS-by-the-numbers (Accessed 12 April 2018). Geneva, Switzerland: Joint United Nations Programme on HIV/AIDS.
-
- Laga M, Manoka A, Kivuvu M, Malele B, Tuliza M, et al. (1993) Non-ulcerative sexually transmitted diseases as risk factors for HIV-1 transmission in women: results from a cohort study. AIDS 7: 95–102. - PubMed
-
- Plummer FA, Simonsen JN, Cameron DW, Ndinya-Achola JO, Kreiss JK, et al. (1991) Cofactors in male-female sexual transmission of human immunodeficiency virus type 1. J Infect Dis 163: 233–239. - PubMed
-
- Ramjee G, Williams B, Gouws E, Van Dyck E, De Deken B, et al. (2005) The impact of incident and prevalent herpes simplex virus-2 infection on the incidence of HIV-1 infection among commercial sex workers in South Africa. J Acquir Immune Defic Syndr 39: 333–339. - PubMed
-
- Stamm WE, Handsfield HH, Rompalo AM, Ashley RL, Roberts PL, et al. (1988) The association between genital ulcer disease and acquisition of HIV infection in homosexual men. JAMA 260: 1429–1433. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
