

Maternal age and offspring developmental vulnerability at age five: A population-based cohort study of Australian children
- PMID: 29689098
- PMCID: PMC5915778
- DOI: 10.1371/journal.pmed.1002558
Maternal age and offspring developmental vulnerability at age five: A population-based cohort study of Australian children
Abstract
Background: In recent decades, there has been a shift to later childbearing in high-income countries. There is limited large-scale evidence of the relationship between maternal age and child outcomes beyond the perinatal period. The objective of this study is to quantify a child's risk of developmental vulnerability at age five, according to their mother's age at childbirth.
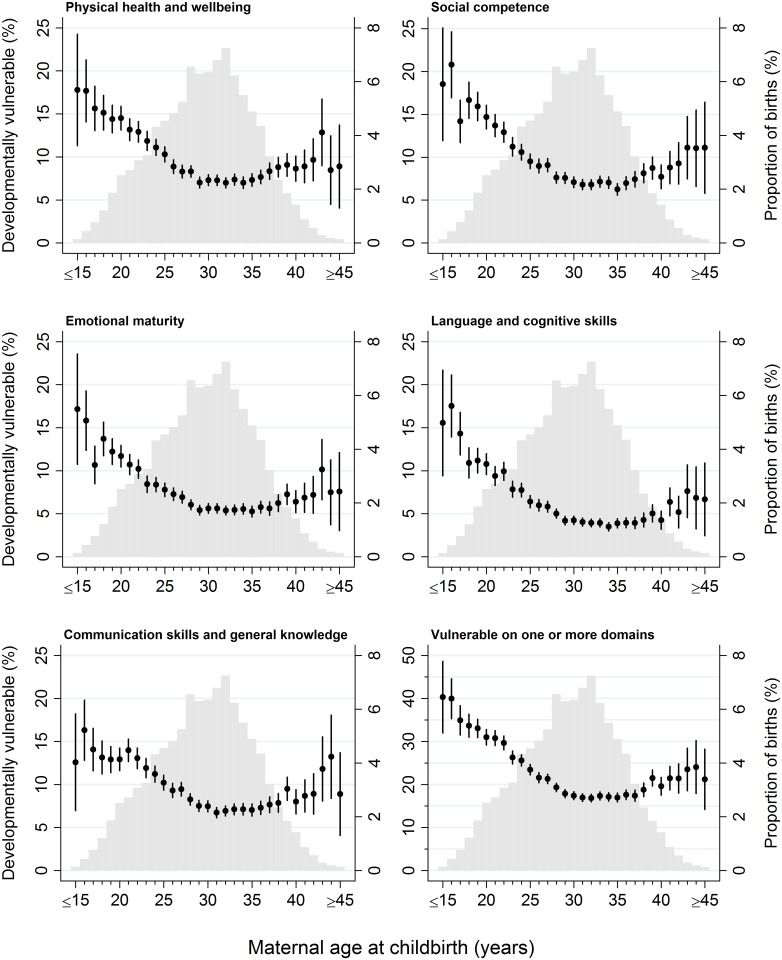
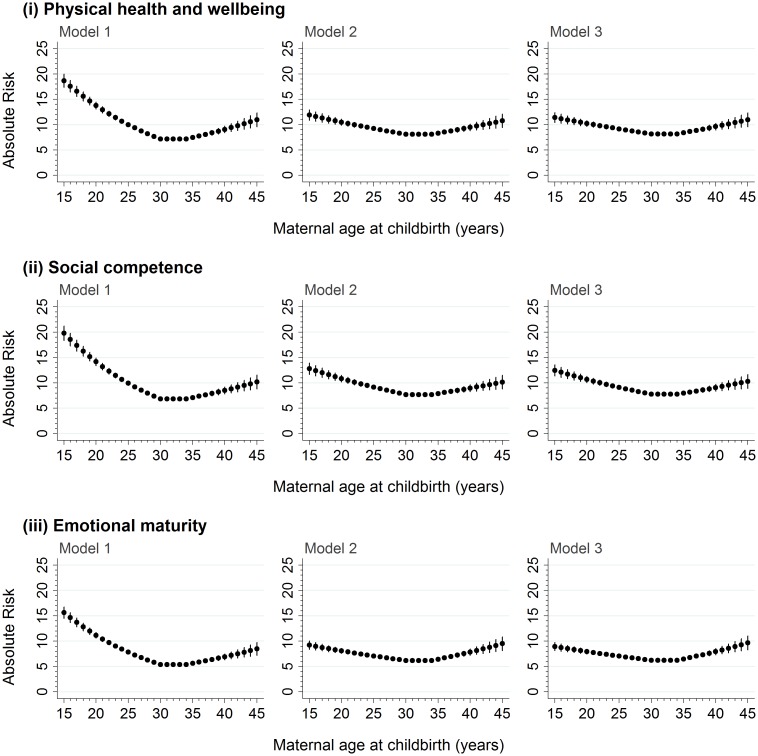
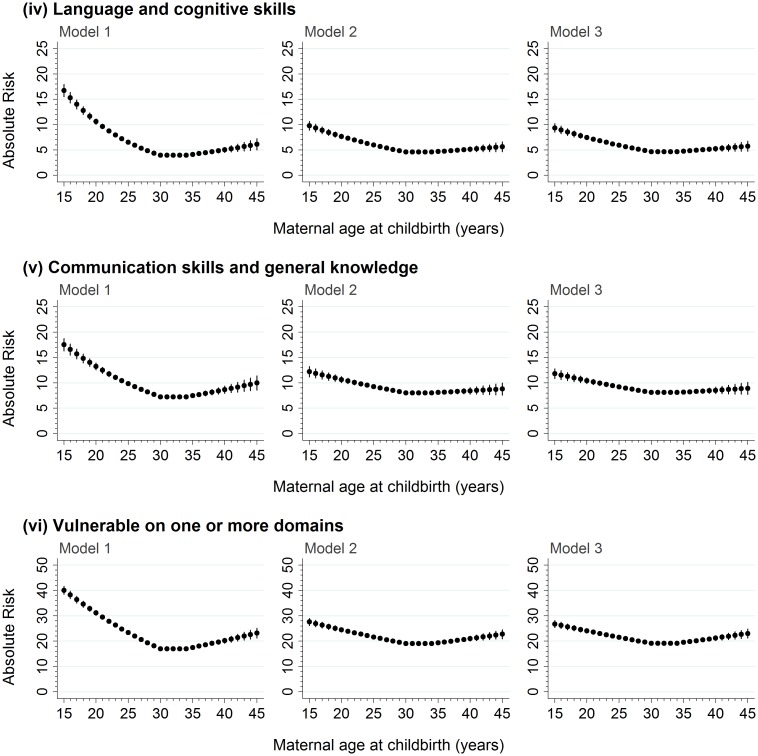
Methods and findings: Linkage of population-level perinatal, hospital, and birth registration datasets to data from the Australian Early Development Census (AEDC) and school enrolments in Australia's most populous state, New South Wales (NSW), enabled us to follow a cohort of 99,530 children from birth to their first year of school in 2009 or 2012. The study outcome was teacher-reported child development on five domains measured by the AEDC, including physical health and well-being, emotional maturity, social competence, language and cognitive skills, and communication skills and general knowledge. Developmental vulnerability was defined as domain scores below the 2009 AEDC 10th percentile cut point. The mean maternal age at childbirth was 29.6 years (standard deviation [SD], 5.7), with 4,382 children (4.4%) born to mothers aged <20 years and 20,026 children (20.1%) born to mothers aged ≥35 years. The proportion vulnerable on ≥1 domains was 21% overall and followed a reverse J-shaped distribution according to maternal age: it was highest in children born to mothers aged ≤15 years, at 40% (95% CI, 32-49), and was lowest in children born to mothers aged between 30 years and ≤35 years, at 17%-18%. For maternal ages 36 years to ≥45 years, the proportion vulnerable on ≥1 domains increased to 17%-24%. Adjustment for sociodemographic characteristics significantly attenuated vulnerability risk in children born to younger mothers, while adjustment for potentially modifiable factors, such as antenatal visits, had little additional impact across all ages. Although the multi-agency linkage yielded a broad range of sociodemographic, perinatal, health, and developmental variables at the child's birth and school entry, the study was necessarily limited to variables available in the source data, which were mostly recorded for administrative purposes.
Conclusions: Increasing maternal age was associated with a lesser risk of developmental vulnerability for children born to mothers aged 15 years to about 30 years. In contrast, increasing maternal age beyond 35 years was generally associated with increasing vulnerability, broadly equivalent to the risk for children born to mothers in their early twenties, which is highly relevant in the international context of later childbearing. That socioeconomic disadvantage explained approximately half of the increased risk of developmental vulnerability associated with younger motherhood suggests there may be scope to improve population-level child development through policies and programs that support disadvantaged mothers and children.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Role of maternal age at birth in child development among Indigenous and non-Indigenous Australian children in their first school year: a population-based cohort study.Lancet Child Adolesc Health. 2020 Jan;4(1):46-57. doi: 10.1016/S2352-4642(19)30334-7. Epub 2019 Nov 19. Lancet Child Adolesc Health. 2020. PMID: 31757762
-
Gestational age and child development at school entry.Sci Rep. 2021 Jul 15;11(1):14522. doi: 10.1038/s41598-021-93701-y. Sci Rep. 2021. PMID: 34267259 Free PMC article.
-
Associations between clusters of early life risk factors and developmental vulnerability at age 5: a retrospective cohort study using population-wide linkage of administrative data in Tasmania, Australia.BMJ Open. 2020 Apr 20;10(4):e033795. doi: 10.1136/bmjopen-2019-033795. BMJ Open. 2020. PMID: 32312726 Free PMC article.
-
Pediatric AIDS and perinatal HIV infection in Zaire: epidemiologic and pathologic findings.Prog AIDS Pathol. 1992;3(1):1-33. Prog AIDS Pathol. 1992. PMID: 1606299 Review.
-
Association Between Maternal Perinatal Depression and Anxiety and Child and Adolescent Development: A Meta-analysis.JAMA Pediatr. 2020 Nov 1;174(11):1082-1092. doi: 10.1001/jamapediatrics.2020.2910. JAMA Pediatr. 2020. PMID: 32926075 Free PMC article.
Cited by
-
Intellectual disabilities and autism among children with congenital heart defects, Western Australia, 1983-2010.BMC Pediatr. 2023 Mar 4;23(1):106. doi: 10.1186/s12887-023-03924-3. BMC Pediatr. 2023. PMID: 36870968 Free PMC article.
-
Associations between maternal folate status and choline intake during pregnancy and neurodevelopment at 3-4 years of age in the Alberta Pregnancy Outcomes and Nutrition (APrON) study.J Dev Orig Health Dis. 2023 Jun;14(3):402-414. doi: 10.1017/S2040174423000041. Epub 2023 Mar 20. J Dev Orig Health Dis. 2023. PMID: 36939090 Free PMC article.
-
Factors Associated with the Suspected Delay in the Language Development of Early Childhood in Southern Thailand.Children (Basel). 2022 May 4;9(5):662. doi: 10.3390/children9050662. Children (Basel). 2022. PMID: 35626839 Free PMC article.
-
Determinants of underweight among HIV-Infected children in pastoral communities of Southern Ethiopia: a facility-based cross-sectional study.BMC Public Health. 2025 May 31;25(1):2027. doi: 10.1186/s12889-025-23275-1. BMC Public Health. 2025. PMID: 40450246 Free PMC article.
-
Use of in vitro fertilization-ethical issues.Ups J Med Sci. 2020 May;125(2):192-199. doi: 10.1080/03009734.2019.1684405. Epub 2019 Nov 5. Ups J Med Sci. 2020. PMID: 31686575 Free PMC article. Review.
References
-
- Organisation for Economic Co-operation and Development (OECD). SF2.3 Age of mothers at childbirth and age-specific fertility; 2016 [cited 2016 Oct 24]. Database: OECD Family Database [Internet]. Available from: http://www.oecd.org/els/family/database.htm
-
- Carolan M. The Graying of the Obstetric Population: Implications for the Older Mother. J Obstet Gynecol Neonatal Nurs. 2003;32(1):19–27. doi: 10.1177/0884217502239797 - DOI - PubMed
-
- Goisis A, Schneider DC, Myrskyla M. The reversing association between advanced maternal age and child cognitive ability: evidence from three UK birth cohorts. Int J Epidemiol. 2017;46(3):850–9. doi: 10.1093/ije/dyw354 - DOI - PMC - PubMed
-
- Tearne JE. Older maternal age and child behavioral and cognitive outcomes: a review of the literature. Fertil Steril. 2015;103(6):1381–91. doi: 10.1016/j.fertnstert.2015.04.027 - DOI - PubMed
-
- Henderson M, Richards M, Stansfeld S, Hotopf M. The association between childhood cognitive ability and adult long-term sickness absence in three British birth cohorts: a cohort study. BMJ Open. 2012;2(2):e000777 doi: 10.1136/bmjopen-2011-000777 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
