

Clinicopathological Characteristics and Mutations Driving Development of Early Lung Adenocarcinoma: Tumor Initiation and Progression
- PMID: 29690599
- PMCID: PMC5979290
- DOI: 10.3390/ijms19041259
Clinicopathological Characteristics and Mutations Driving Development of Early Lung Adenocarcinoma: Tumor Initiation and Progression
Abstract
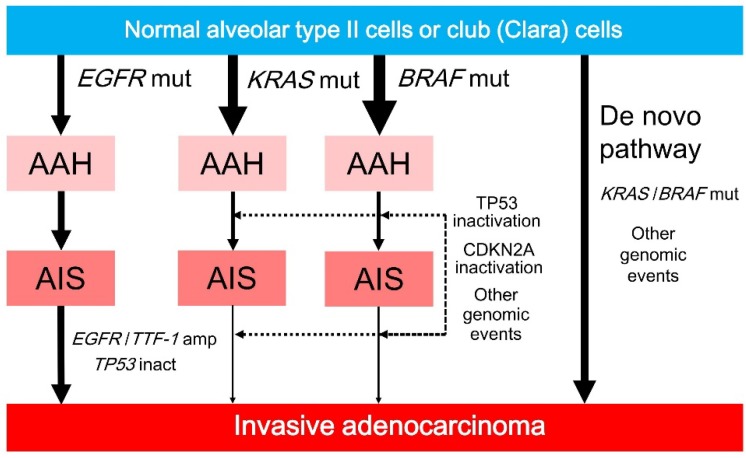
Lung cancer is the leading cause of cancer-related deaths worldwide, with lung adenocarcinoma representing the most common lung cancer subtype. Among all lung adenocarcinomas, the most prevalent subset develops via tumorigenesis and progression from atypical adenomatous hyperplasia (AAH) to adenocarcinoma in situ (AIS), to minimally invasive adenocarcinoma (MIA), to overt invasive adenocarcinoma with a lepidic pattern. This stepwise development is supported by the clinicopathological and molecular characteristics of these tumors. In the 2015 World Health Organization classification, AAH and AIS are both defined as preinvasive lesions, whereas MIA is identified as an early invasive adenocarcinoma that is not expected to recur if removed completely. Recent studies have examined the molecular features of lung adenocarcinoma tumorigenesis and progression. EGFR-mutated adenocarcinoma frequently develops via the multistep progression. Oncogene-induced senescence appears to decrease the frequency of the multistep progression in KRAS- or BRAF-mutated adenocarcinoma, whose tumor evolution may be associated with epigenetic alterations and kinase-inactive mutations. This review summarizes the current knowledge of tumorigenesis and tumor progression in early lung adenocarcinoma, with special focus on its clinicopathological characteristics and their associations with driver mutations (EGFR, KRAS, and BRAF) as well as on its molecular pathogenesis and progression.
Keywords: CDKN2A (p16); HNF4A; NKX2-1 (TTF-1) amplification; Napsin A; Noguchi classification; TP53 (p53); de novo pathway; immunohistochemistry; molecular pathological epidemiology; terminal respiratory unit (TRU)-lineage.
Conflict of interest statement
The author declares no conflict of interest.
Figures



References
-
- Travis W.D., Brambilla E., Burke A.P., Marx A., Nicholson A.G. WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart. 4th ed. IARC; Lyon, France: 2015. - PubMed
-
- Travis W.D., Brambilla E., Noguchi M., Nicholson A.G., Geisinger K.R., Yatabe Y., Beer D.G., Powell C.A., Riely G.J., van Schil P.E., et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J. Thorac. Oncol. 2011;6:244–285. doi: 10.1097/JTO.0b013e318206a221. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
