

Readmission Patterns Over 90-Day Episodes of Care Among Medicare Fee-for-Service Beneficiaries Discharged to Post-acute Care
- PMID: 29691152
- PMCID: PMC6165689
- DOI: 10.1016/j.jamda.2018.03.006
Readmission Patterns Over 90-Day Episodes of Care Among Medicare Fee-for-Service Beneficiaries Discharged to Post-acute Care
Abstract
Objective: Examine readmission patterns over 90-day episodes of care in persons discharged from hospitals to post-acute settings.
Design: Retrospective cohort study.
Setting: Acute care hospitals.
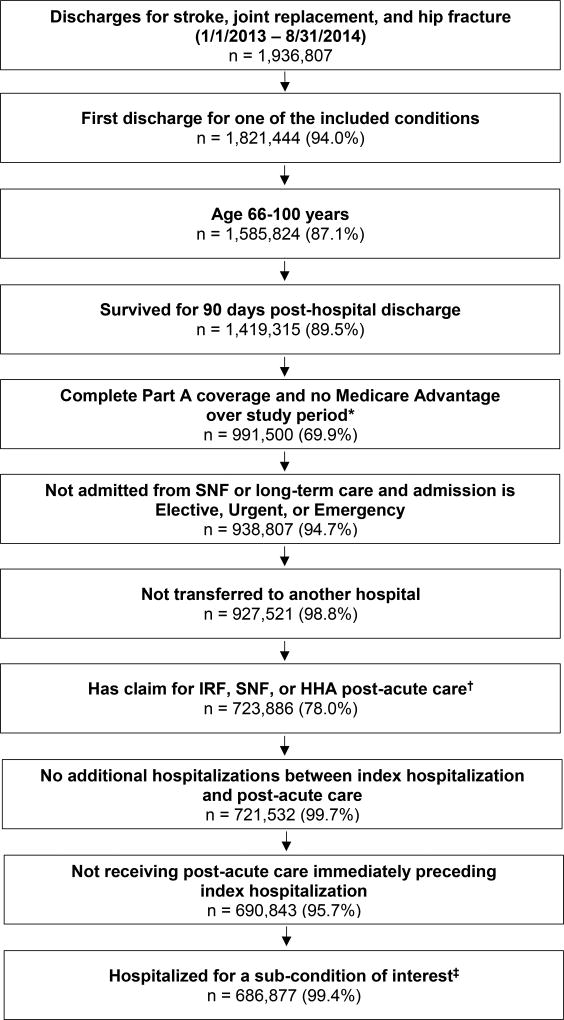
Participants: Medicare fee-for-service enrollees (N = 686,877) discharged from hospitals to post-acute care in 2013-2014. The cohort included beneficiaries >65 years of age hospitalized for stroke, joint replacement, or hip fracture and who survived for 90 days following discharge.
Measurements: 90-day unplanned readmissions.
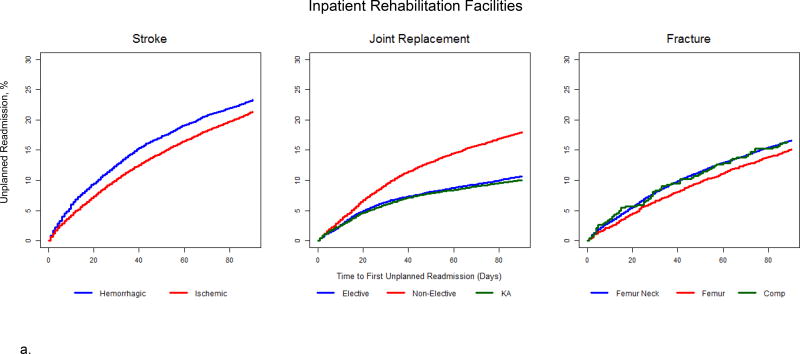
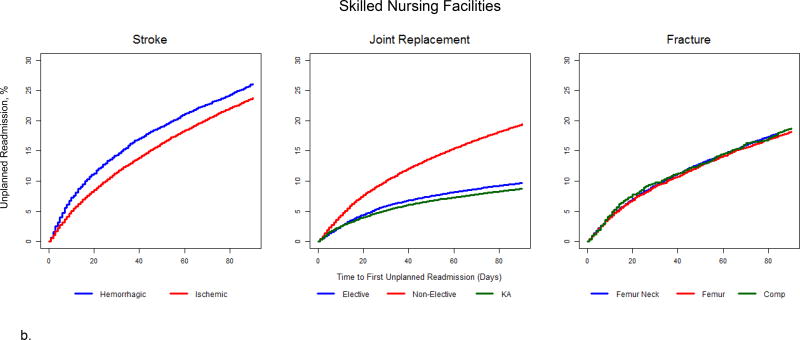
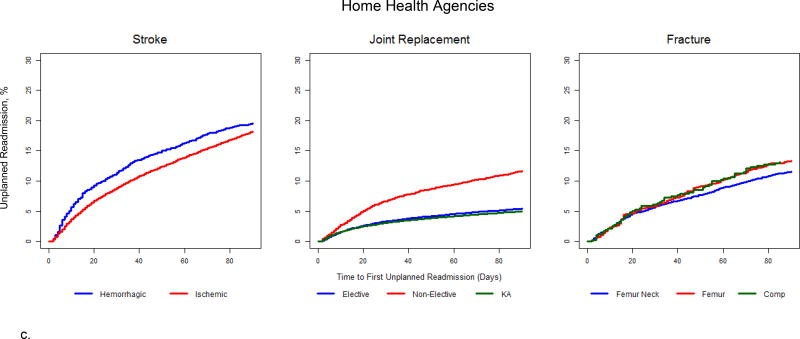
Results: The cohort included 127,680 individuals with stroke, 442,195 undergoing joint replacement, and 117,002 with hip fracture. Thirty-day readmission rates ranged from 3.1% for knee replacement patients discharged to home health agencies (HHAs) to 14.4% for hemorrhagic stroke patients discharged to skilled nursing facilities (SNFs). Ninety-day readmission rates ranged from 5.0% for knee replacement patients discharged to HHAs to 26.1% for hemorrhagic stroke patients discharged to SNFs. Differences in readmission rates decreased between stroke subconditions (hemorrhagic and ischemic) and increased between joint replacement subconditions (knee, elective hip, and nonelective hip) from 30 to 90 days across all initial post-acute discharge settings.
Conclusions: We observed clear patterns in readmissions over 90-day episodes of care across post-acute discharge settings and subconditions. Our findings suggest that patients with hemorrhagic stroke may be more vulnerable than those with ischemic over the first 30 days after hospital discharge. For patients receiving nonelective joint replacements, readmission prevention efforts should start immediately after discharge and continue, or even increase, over the 90-day episode of care.
Keywords: Quality of care; health care reform; health services research; outcomes research.
Copyright © 2018 AMDA – The Society for Post-Acute and Long-Term Care Medicine. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to report.
Figures
References
-
- Burwell SM. Setting value-based payment goals--HHS efforts to improve U.S. health care. N Engl J Med. 2015;372(10):897–899. - PubMed
-
- The Lewin Group. [Accessed July 5, 2017];CMS Bundled Payments for Care Improvement (BPCI) Initiative Models 2–4: Year 1 Evaluation & Monitoring Annual Report. https://innovation.cms.gov/Files/reports/BPCI-EvalRpt1.pdf.
-
- Department of Health and Human Services. [Accessed July 5, 2017];Centers for Medicare & Medicaid Services. Federal Register. Medicare Program; Comprehensive Care for Joint Replacement Payment Model for Acute Care Hospitals Furnishing Lower Extremity Joint Replacement Services; Final Rule. https://www.gpo.gov/fdsys/pkg/FR-2015-11-24/pdf/2015-29438.pdf. - PubMed
-
- Department of Health and Human Services. [Accessed December 16, 2017];Federal Register. Medicare Program; Advancing Care Coordination Through Episode Payment Models (EPMs); Cardiac Rehabilitation Incentive Payment Model; and Changes to the Comprehensive Care for Joint Replacement Model (CJR); Proposed Rule. https://www.gpo.gov/fdsys/pkg/FR-2016-08-02/pdf/2016-17733.pdf. - PubMed
-
- Medicare Payment Advisory Commission. [Accessed July 20, 2016];A Data Book: Health Care Spending and the Medicare Program. 2016 Jun; http://medpac.gov/documents/data-book/june-2016-data-book-health-care-sp....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
