

Non-invasive detection of human cardiomyocyte death using methylation patterns of circulating DNA
- PMID: 29691397
- PMCID: PMC5915384
- DOI: 10.1038/s41467-018-03961-y
Non-invasive detection of human cardiomyocyte death using methylation patterns of circulating DNA
Abstract
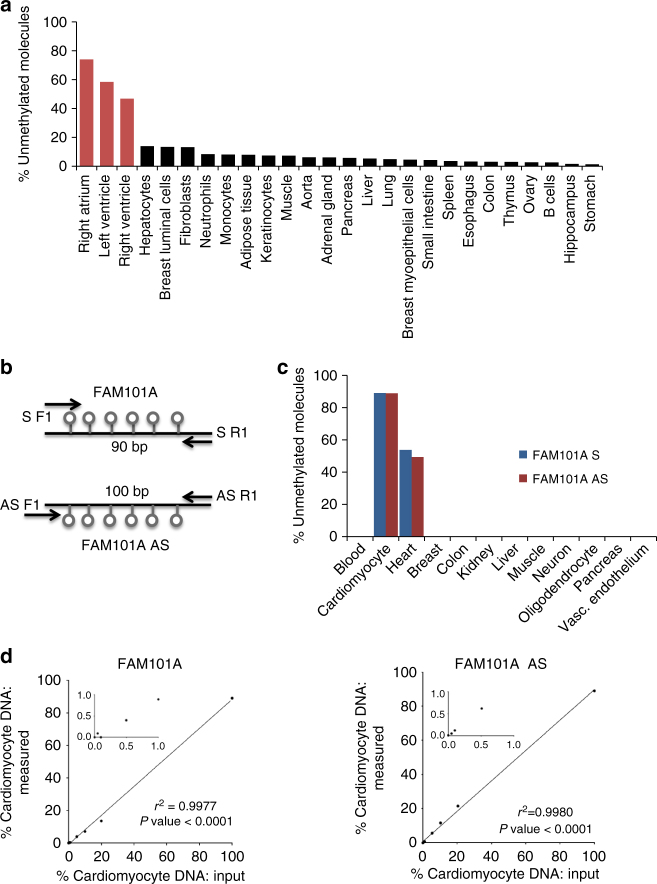
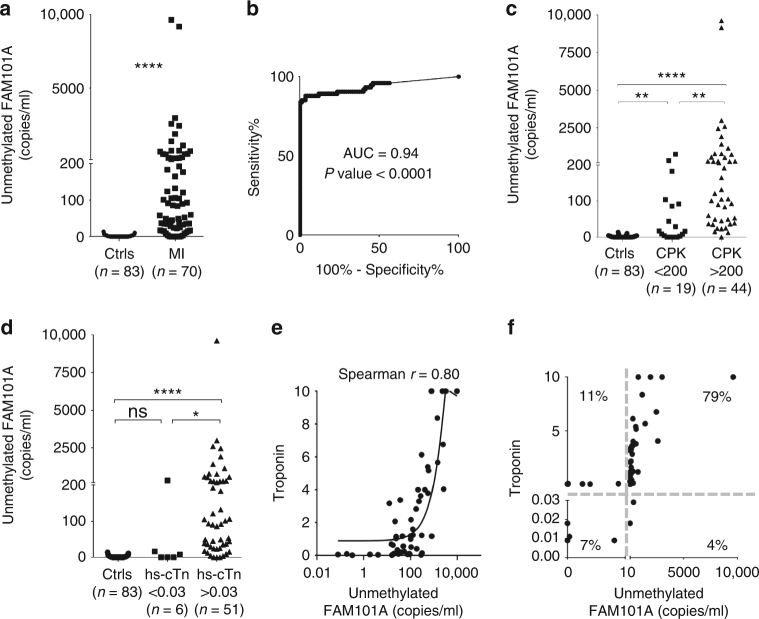
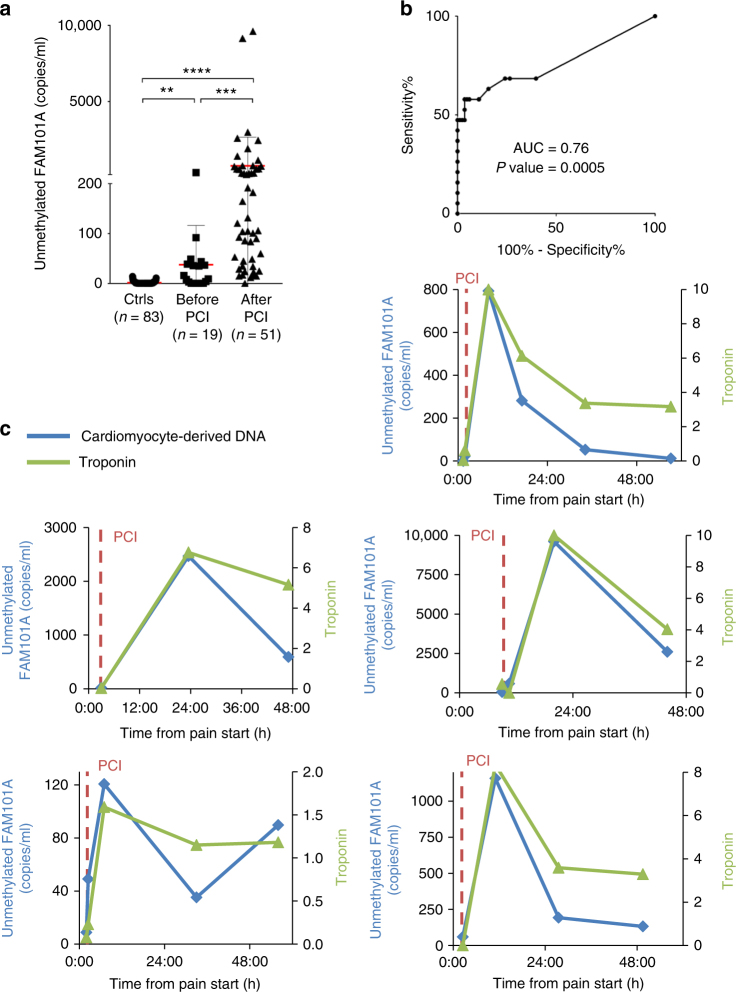
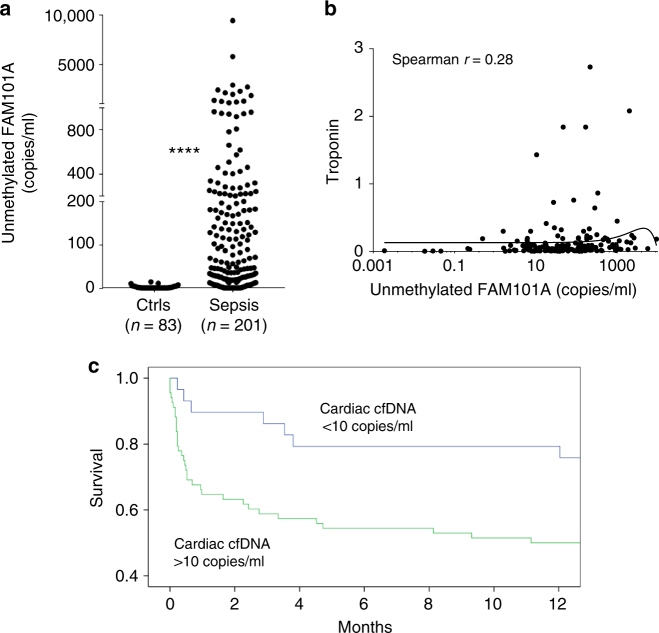
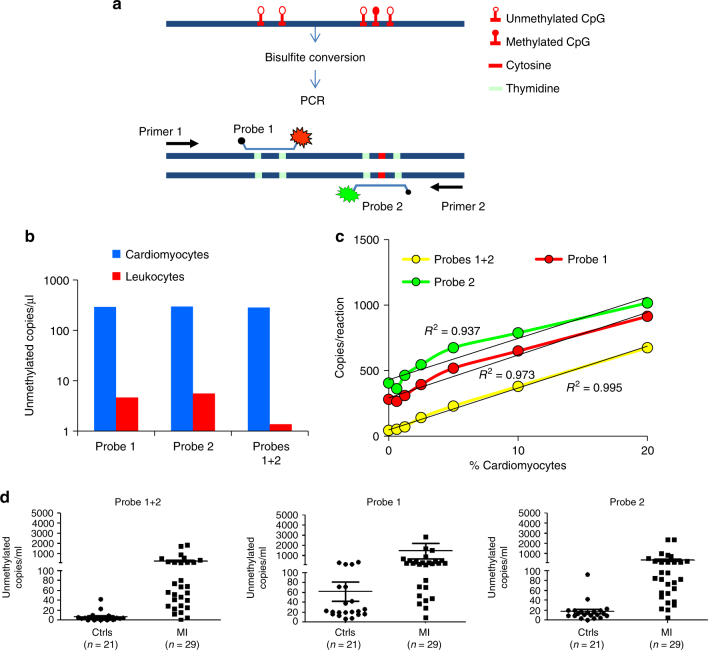
Detection of cardiomyocyte death is crucial for the diagnosis and treatment of heart disease. Here we use comparative methylome analysis to identify genomic loci that are unmethylated specifically in cardiomyocytes, and develop these as biomarkers to quantify cardiomyocyte DNA in circulating cell-free DNA (cfDNA) derived from dying cells. Plasma of healthy individuals contains essentially no cardiomyocyte cfDNA, consistent with minimal cardiac turnover. Patients with acute ST-elevation myocardial infarction show a robust cardiac cfDNA signal that correlates with levels of troponin and creatine phosphokinase (CPK), including the expected elevation-decay dynamics following coronary angioplasty. Patients with sepsis have high cardiac cfDNA concentrations that strongly predict mortality, suggesting a major role of cardiomyocyte death in mortality from sepsis. A cfDNA biomarker for cardiomyocyte death may find utility in diagnosis and monitoring of cardiac pathologies and in the study of normal human cardiac physiology and development.
Conflict of interest statement
Ju.M., R.S., B.G. and Y.D. are inventors on a patent entitled “A Novel approach for improving the detection of tissue-specific DNA: Sense and Antisense strands of bisulfite treated DNA” (patent number 62/531,990), and a patent entitled “A dual-probe digital droplet PCR strategy for specific detection of tissue-specific circulating DNA molecules” (patent number 62/531,983); H.Z., Ju.M., Jo.M., D.N., R.S., B.G. and Y.D. are inventors on a patent entitled “New set of probes for determining tissue of origin by methylation pattern” (patent number 62/531,988). The remaining authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
