

My patient has received fluid. How to assess its efficacy and side effects?
- PMID: 29691755
- PMCID: PMC5915982
- DOI: 10.1186/s13613-018-0400-z
My patient has received fluid. How to assess its efficacy and side effects?
Abstract
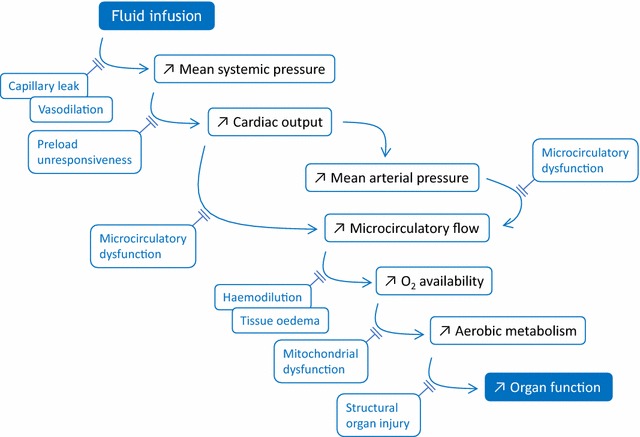
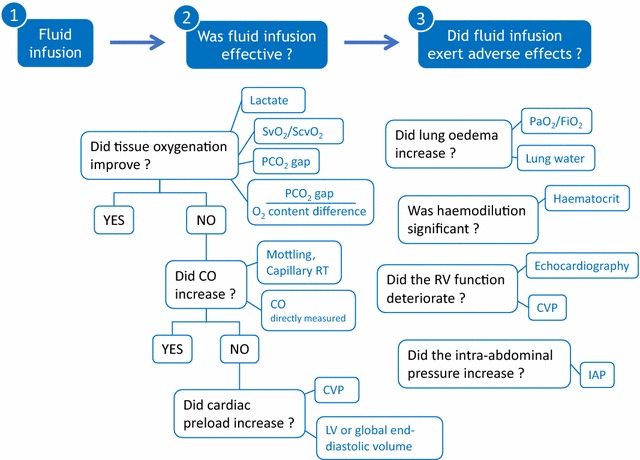
Many efforts have been made to predict, before giving fluid, whether it will increase cardiac output. Nevertheless, after fluid administration, it is also essential to assess the therapeutic efficacy and to look for possible adverse effects. Like for any drug, this step should not be missed. Basically, volume expansion is aimed at improving tissue oxygenation and organ function. To assess this final result, clinical signs are often unhelpful. The increase in urine output in case of acute kidney injury is a poor marker of the kidney perfusion improvement. Even if oxygen delivery has increased with fluid, the increase in oxygen consumption is not constant. Assessing this response needs to measure markers such as lactate, central/mixed venous oxygen saturation, or carbon dioxide-derived indices. If tissue oxygenation did not improve, one should check that cardiac output has actually increased with fluid administration. To assess this response, changes in arterial pressure are not reliable enough, and direct measurements of cardiac output are required. In cases where cardiac output did not increase with fluid, one should check that it was not due to an insufficient volume of fluid administered. For this purpose, volume markers of cardiac preload sometimes lack precision. The central venous pressure, in theory at least, should not augment to a large extent in fluid responders. The worst adverse effect of fluids is the increase in the cumulative fluid balance. In patients with acute respiratory distress syndrome (ARDS), the risk of aggravating pulmonary oedema should be systematically assessed by looking for increases in extravascular lung water, or, more indirectly, increases in central venous or pulmonary artery occlusion pressure. In ARDS patients receiving fluid, one should always keep in mind the risk of inducing/aggravating right ventricular dilation, which should be confirmed through echocardiography. The risk of increasing the intra-abdominal pressure should be carefully sought in patients at risk. Finally, fluid-induced haemodilution should not be neglected. Like for any drug which has inconsistent effectiveness and may exert significant harm, the correct fluid management should include a cautious and comprehensive assessment of fluid-induced benefits and side effects.
Keywords: Cardiac output; Extravascular lung water; Fluid challenge; Fluid responsiveness; Passive leg raising; Pulse pressure variation.
Figures
Similar articles
-
How I personalize fluid therapy in septic shock?Crit Care. 2023 Mar 24;27(1):123. doi: 10.1186/s13054-023-04363-3. Crit Care. 2023. PMID: 36964573 Free PMC article. Review.
-
[Pulse indicator continuous cardiac output measurement-guided treatment aids two pediatric patients with severe acute pancreatitis complicated with acute respiratory distress syndrome].Zhonghua Er Ke Za Zhi. 2014 Sep;52(9):693-8. Zhonghua Er Ke Za Zhi. 2014. PMID: 25476433 Chinese.
-
[Experts consensus on the management of the right heart function in critically ill patients].Zhonghua Nei Ke Za Zhi. 2017 Dec 1;56(12):962-973. doi: 10.3760/cma.j.issn.0578-1426.2017.12.017. Zhonghua Nei Ke Za Zhi. 2017. PMID: 29202543 Chinese.
-
Lactate and venoarterial carbon dioxide difference/arterial-venous oxygen difference ratio, but not central venous oxygen saturation, predict increase in oxygen consumption in fluid responders.Crit Care Med. 2013 Jun;41(6):1412-20. doi: 10.1097/CCM.0b013e318275cece. Crit Care Med. 2013. PMID: 23442986
-
How can assessing hemodynamics help to assess volume status?Intensive Care Med. 2022 Oct;48(10):1482-1494. doi: 10.1007/s00134-022-06808-9. Epub 2022 Aug 10. Intensive Care Med. 2022. PMID: 35945344 Free PMC article. Review.
Cited by
-
Role of Crystalloids in the Perioperative Setting: From Basics to Clinical Applications and Enhanced Recovery Protocols.J Clin Med. 2023 Sep 12;12(18):5930. doi: 10.3390/jcm12185930. J Clin Med. 2023. PMID: 37762871 Free PMC article. Review.
-
Hemodynamic management of septic shock: beyond the Surviving Sepsis Campaign guidelines.Clin Exp Emerg Med. 2023 Sep;10(3):255-264. doi: 10.15441/ceem.23.065. Epub 2023 Jul 13. Clin Exp Emerg Med. 2023. PMID: 37439141 Free PMC article.
-
Volumetric Monitoring and Extravascular Lung Water in Perioperative Setting and Critically Ill.Turk J Anaesthesiol Reanim. 2021 Jun;49(3):201-210. doi: 10.5152/TJAR.2021.21382. Turk J Anaesthesiol Reanim. 2021. PMID: 35110139 Free PMC article.
-
Systematic assessment of fluid responsiveness during early septic shock resuscitation: secondary analysis of the ANDROMEDA-SHOCK trial.Crit Care. 2020 Jan 23;24(1):23. doi: 10.1186/s13054-020-2732-y. Crit Care. 2020. PMID: 31973735 Free PMC article.
-
Association of fluid balance with mortality in sepsis is modified by admission hemoglobin levels: A large database study.PLoS One. 2021 Jun 14;16(6):e0252629. doi: 10.1371/journal.pone.0252629. eCollection 2021. PLoS One. 2021. PMID: 34125858 Free PMC article.
References
-
- Monnet X, Julien F, Ait-Hamou N, Lequoy M, Gosset C, Jozwiak M, et al. Lactate and venoarterial carbon dioxide difference/arterial-venous oxygen difference ratio, but not central venous oxygen saturation, predict increase in oxygen consumption in fluid responders. Crit Care Med. 2013;41:1412–1420. doi: 10.1097/CCM.0b013e318275cece. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
