

Glucocorticoid-induced osteoporosis: an update
- PMID: 29691807
- PMCID: PMC5997116
- DOI: 10.1007/s12020-018-1588-2
Glucocorticoid-induced osteoporosis: an update
Abstract
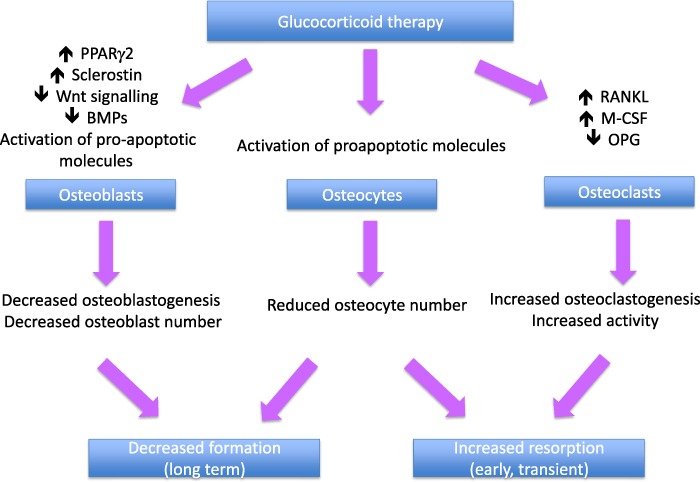
Glucocorticoid-induced osteoporosis is the most common secondary cause of osteoporosis and the resulting fractures cause significant morbidity. Following initiation of oral glucocorticoids, rapid bone loss occurs, and fracture risk increases within a few months in a dose-dependent manner. These adverse effects are due to inhibition of bone formation accompanied by an early but transient increase in bone resorption. Multiple mechanisms underlie these changes in bone remodeling; direct effects include upregulation of PPARγR2, increased expression of sclerostin and increased RANKL/OPG ratio, whilst hypogonadism, altered renal and intestinal calcium handling, and reduced production of insulin-like growth factor 1 also contribute. Fracture risk assessment should be performed as soon as possible after glucocorticoids are initiated and bone protective therapy started promptly in individuals at high-risk, with calcium and vitamin D supplements where appropriate. Oral bisphosphonates are currently regarded as first line options on the grounds of their low cost. However, teriparatide has been shown to be superior in its effects on BMD and vertebral fracture risk in glucocorticoid-treated individuals with osteoporosis and should be considered as an alternative first line option in high-risk patients.
Keywords: Bisphosphonates; Bone density; Fracture; Glucocorticoids; Teriparatide.
Conflict of interest statement
Prof Compston has received advisory and speaking fees from Gilead and speaking fees from Amgen and UCB.
Figures
References
-
- Silverman S, Curtis J, Saag K, Flahive J, Adachi J, Anderson F, Chapurlat R, Cooper C, Diez-Perez A, Greenspan S, Hooven F, Le Croix A, March L, Netelenbos JC, Nieves J, Pfeilschifter J, Rossini M, Roux C, Siris E, Watts N, Compston J. International management of bone health in glucocorticoid-exposed individuals in the observational GLOW study. Osteoporos. Int. 2015;26(1):419–420. doi: 10.1007/s00198-014-2883-2. - DOI - PMC - PubMed
-
- van Staa T, Leufkens HGM, Abenhaim L, Zhang B, Cooper C. Use of oral corticosteroids and risk of fractures. J. Bone Miner. Res. 2000;15:933–1000. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
