

Diagnostic and Treatment Monitoring Potential of A Stool-Based Quantitative Polymerase Chain Reaction Assay for Pulmonary Tuberculosis
- PMID: 29692304
- PMCID: PMC6090360
- DOI: 10.4269/ajtmh.18-0004
Diagnostic and Treatment Monitoring Potential of A Stool-Based Quantitative Polymerase Chain Reaction Assay for Pulmonary Tuberculosis
Abstract
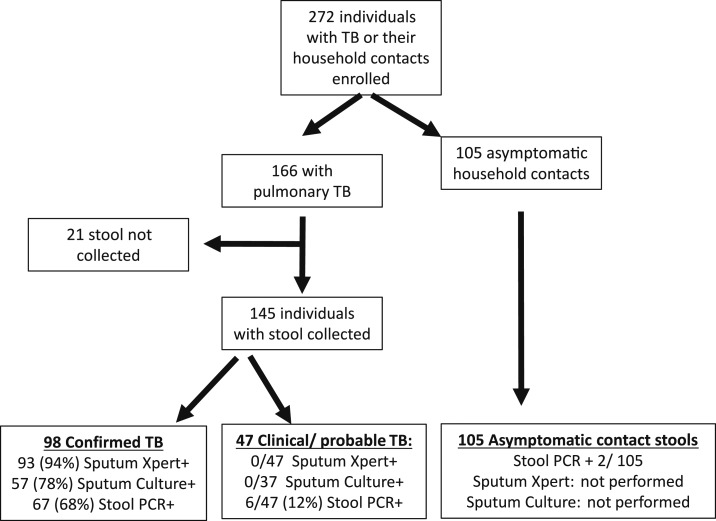
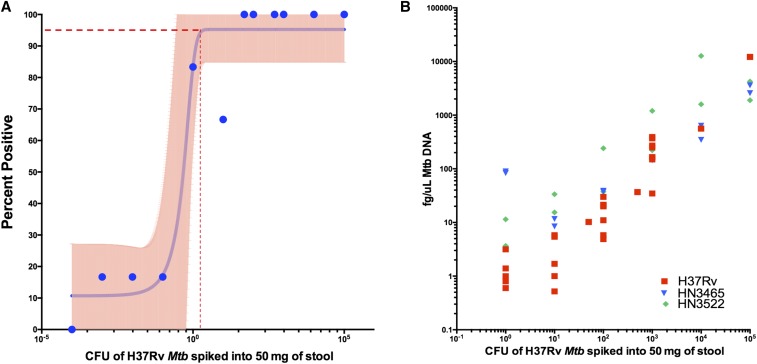
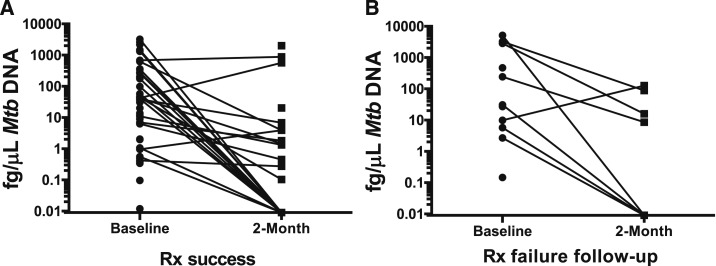
A quantifiable, stool-based, Mycobacterium tuberculosis (Mtb) test has potential complementary value to respiratory specimens. Limit of detection (LOD) was determined by spiking control stool. Clinical test performance was evaluated in a cohort with pulmonary tuberculosis (TB) (N = 166) and asymptomatic household TB child contacts (N = 105). Stool-quantitative polymerase chain reaction (qPCR) results were compared with sputum acid-fast bacilli (AFB) microscopy, GeneXpert MTB/RIF (Xpert MTB/RIF), and cultures. In Mtb stool-spiking studies, the LOD was 96 colony-forming units/50 mg of stool (95% confidence interval [CI]: 84.8-105.6). Among specimens collected within 72 hours of antituberculosis treatment (ATT) initiation, stool qPCR detected 22 of 23 (95%) of culture-positive cases. Among clinically diagnosed cases that were Xpert MTB/RIF and culture negative, stool qPCR detected an additional 8% (3/37). Among asymptomatic, recently TB-exposed participants, stool PCR detected Mtb in two of 105 (1.9%) patients. Two months after ATT, the Mtb quantitative burden in femtogram per microliters decreased (Wilcoxon signed-rank P < 0.001) and persistent positive stool PCR was associated with treatment failure or drug resistance (relative risk 2.8, CI: 1.2-6.5; P = 0.012). Stool-based qPCR is a promising complementary technique to sputum-based diagnosis. It detects and quantifies low levels of stool Mtb DNA, thereby supporting adjunct diagnosis and treatment monitoring in pulmonary TB.
Figures
Comment in
-
The Potential for Testing Stool to Reduce Tuberculosis Missed Diagnoses and Misdiagnoses.Am J Trop Med Hyg. 2018 Aug;99(2):243-245. doi: 10.4269/ajtmh.18-0507. Am J Trop Med Hyg. 2018. PMID: 30076698 Free PMC article. No abstract available.
References
-
- WHO , 2016. Global Tuberculosis Report 2016. Geneva, Switzerland: World Health Organization.
-
- Harries AD, Hargreaves NJ, Kemp J, Jindani A, Enarson DA, Maher D, Salaniponi FM, 2001. Deaths from tuberculosis in sub-Saharan African countries with a high prevalence of HIV-1. Lancet 357: 1519–1523. - PubMed
-
- Harries AD, Nyirenda TE, Banerjee A, Boeree MJ, Salaniponi FM, 1999. Treatment outcome of patients with smear-negative and smear-positive pulmonary tuberculosis in the National Tuberculosis Control Programme, Malawi. Trans R Soc Trop Med Hyg 93: 443–446. - PubMed
-
- Perez-Velez CM, Marais BJ, 2012. Tuberculosis in children. N Engl J Med 367: 348–361. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
