

Absence of Association between Preoperative Estimated Glomerular Filtration Rates and Postoperative Outcomes following Elective Gastrointestinal Surgeries: A Prospective Cohort Study
- PMID: 29692807
- PMCID: PMC5859863
- DOI: 10.1155/2018/5710641
Absence of Association between Preoperative Estimated Glomerular Filtration Rates and Postoperative Outcomes following Elective Gastrointestinal Surgeries: A Prospective Cohort Study
Abstract
Background: Preoperative risk stratification and optimising care of patients undergoing elective surgery are important to reduce the risk of postoperative outcomes. Renal dysfunction is becoming increasingly prevalent, but its impact on patients undergoing elective gastrointestinal surgery is unknown although much evidence is available for cardiac surgery. This study aimed to investigate the impact of preoperative estimated glomerular filtration rate (eGFR) and postoperative outcomes in patients undergoing elective gastrointestinal surgeries.
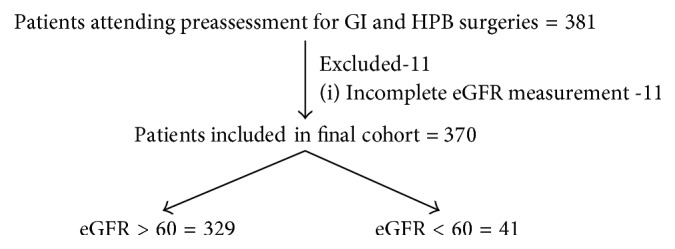
Methods: This prospective study included consecutive adult patients undergoing elective gastrointestinal surgeries attending preassessment screening (PAS) clinics at the Queen Elizabeth Hospital Birmingham (QEHB) between July and August 2016. Primary outcome measure was 30-day overall complication rates and secondary outcomes were grade of complications, 30-day readmission rates, and postoperative care setting.
Results: This study included 370 patients, of which 11% (41/370) had eGFR of <60 ml/min/1.73 m2. Patients with eGFR < 60 ml/min/1.73 m2 were more likely to have ASA grade 3/4 (p < 0.001) and >2 comorbidities (p < 0.001). Overall complication rates were 15% (54/370), with no significant difference in overall (p=0.644) and major complication rates (p=0.831) between both groups. In adjusted models, only surgery grade was predictive of overall complications. Preoperative eGFR did not impact on overall complications (HR: 0.89, 95% CI: 0.45-1.54; p=0.2).
Conclusions: Preoperative eGFR does not appear to impact on postoperative complications in patients undergoing elective gastrointestinal surgeries, even when stratified by surgery grade. These findings will help preassessment clinics in risk stratification and optimisation of perioperative care of patients.
References
-
- Matsushita K., van der Velde M., Astor B. C., et al. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. The Lancet. 2010;375(9731):2073–2081. doi: 10.1016/s0140-6736(10)60674-5. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
