

Establishing a Reproducible Murine Animal Model of Single Anastomosis Duodenoileal Bypass with Sleeve Gastrectomy (SADl-S)
- PMID: 29693220
- PMCID: PMC6018587
- DOI: 10.1007/s11695-018-3254-4
Establishing a Reproducible Murine Animal Model of Single Anastomosis Duodenoileal Bypass with Sleeve Gastrectomy (SADl-S)
Erratum in
-
Correction to: Establishing a Reproducible Murine Animal Model of Single Anastomosis Duodenoileal Bypass with Sleeve Gastrectomy (SADl-S).Obes Surg. 2018 Oct;28(10):3360. doi: 10.1007/s11695-018-3302-0. Obes Surg. 2018. PMID: 29766352 Free PMC article.
Abstract
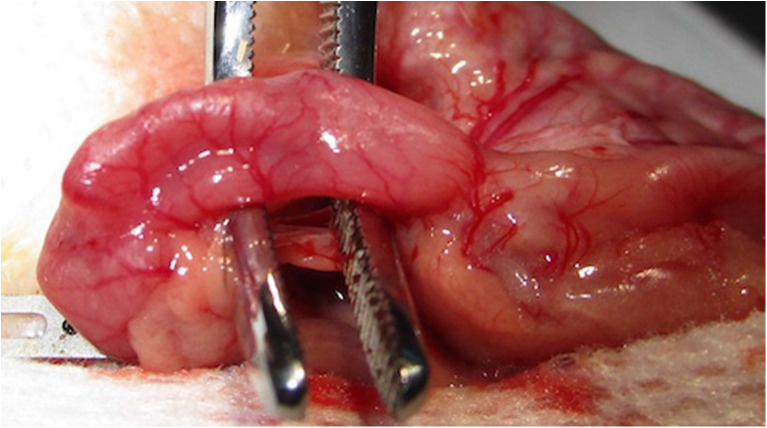
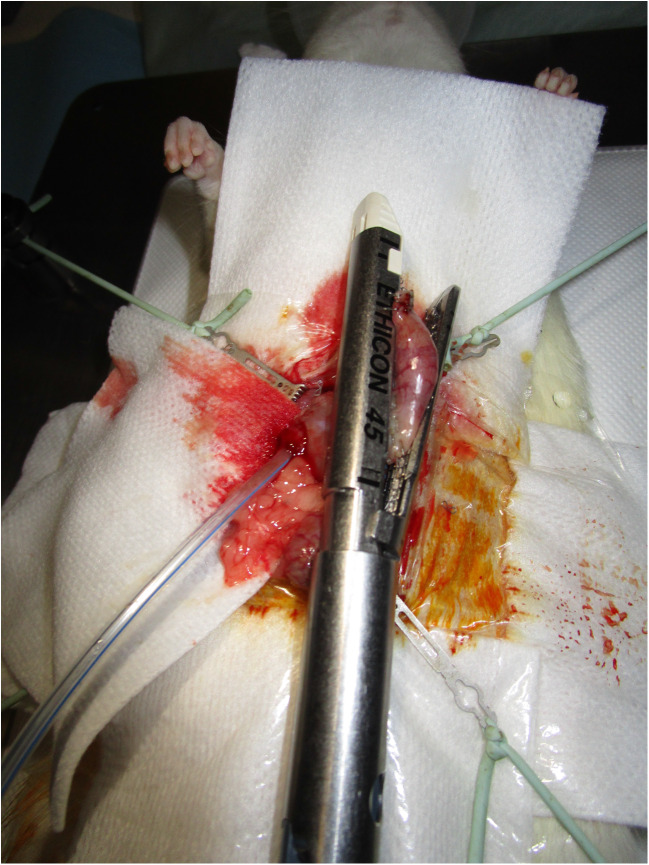
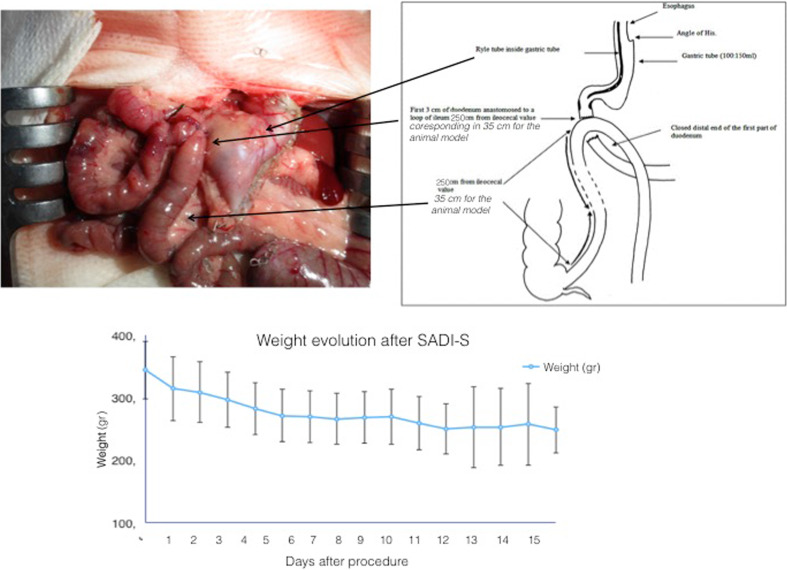
Single-anastomosis duodenoileal bypass with sleeve gastrectomy (SADI-S) is a simplified biliopancreatic diversion. The objective of this study was to develop a reproducible animal model for SADI-S. We used three techniques for duodenal exclusion and duodenoileal anastomosis: (a) surgical clip and side-to-side anastomosis, (b) ligation and side-to-side anastomosis and (c) sectioning the duodenum, closing the duodenal stump and end-to-side anastomosis. We recorded the surgical technique and complications for each method. Twenty-five of 31 rats survived to the end of the study period. One death occurred from accidental anaesthesia overdose and the others from anastomosis leak. Four duodenal exclusions had repermeabilised at necropsy. Our murine model of SADI-S can be consistently reproduced. Sectioning the duodenum is preferable to avoid repermeabilisation of the duodenum.
Keywords: Animal models; Biliopancreatic diversion; Duodenal switch; Metabolic surgery; SADI-S.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Sanchez-Pernaute A, Rubio Herrera MA, Perez-Aguirre E, Garcia Perez JC, Cabrerizo L, Diez Valladares L, Fernandez C, Talavera P, Torres A. Proximal duodenal-ileal end-to-side bypass with sleeve gastrectomy: proposed technique. Obes Surg. 2007;17(12):1614–1618. doi: 10.1007/s11695-007-9287-8. - DOI - PubMed
-
- Stenberg E, Szabo E, Agren G, Ottosson J, Marsk R, Lonroth H, Boman L, Magnuson A, Thorell A, Naslund I. Closure of mesenteric defects in laparoscopic gastric bypass: a multicentre, randomised, parallel, open-label trial. Lancet. 2016;387(10026):1397–1404. doi: 10.1016/S0140-6736(15)01126-5. - DOI - PubMed
-
- Rubino F, Forgione A, Cummings DE, Vix M, Gnuli D, Mingrone G, Castagneto M, Marescaux J. The mechanism of diabetes control after gastrointestinal bypass surgery reveals a role of the proximal small intestine in the pathophysiology of type 2 diabetes. Ann Surg. 2006;244(5):741–749. doi: 10.1097/01.sla.0000224726.61448.1b. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
