

Brief Report: Circulating Cytokine Profiles and Antineutrophil Cytoplasmic Antibody Specificity in Patients With Antineutrophil Cytoplasmic Antibody-Associated Vasculitis
- PMID: 29693324
- PMCID: PMC6093207
- DOI: 10.1002/art.40471
Brief Report: Circulating Cytokine Profiles and Antineutrophil Cytoplasmic Antibody Specificity in Patients With Antineutrophil Cytoplasmic Antibody-Associated Vasculitis
Abstract
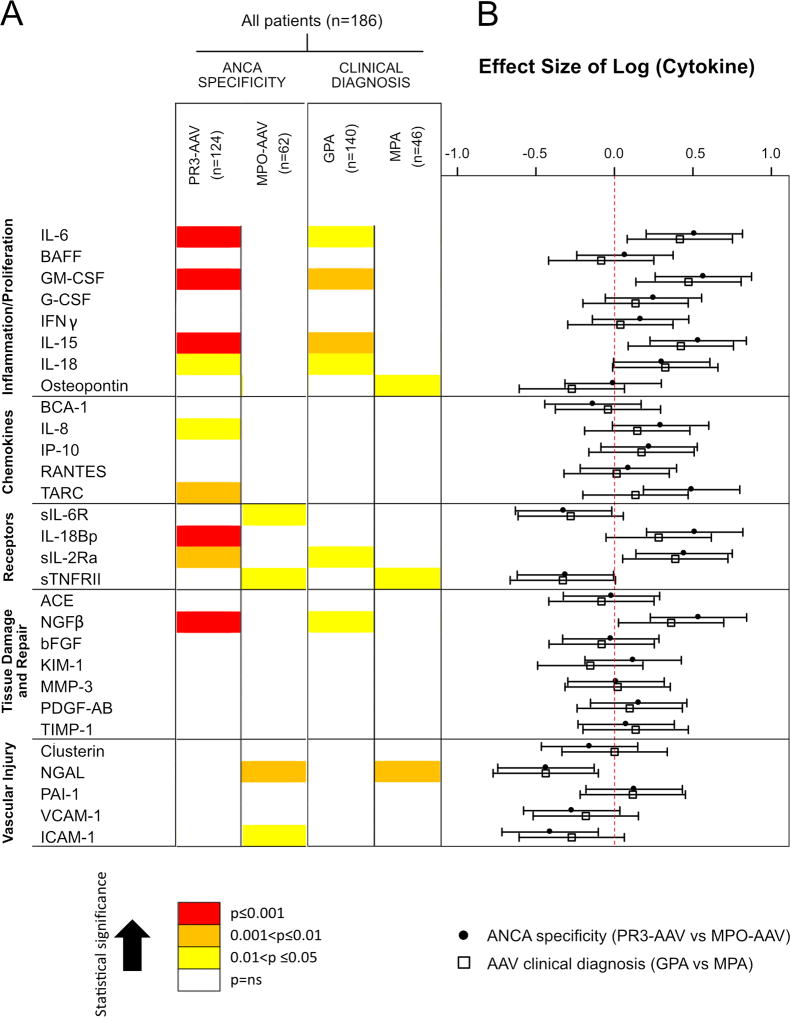
Objective: To evaluate circulating cytokine profiles in patients with antineutrophil cytoplasmic antibody-associated vasculitis (AAV), classified by antineutrophil cytoplasmic antibody (ANCA) specificity (proteinase 3 ANCA [PR3-ANCA] versus myeloperoxidase ANCA [MPO-ANCA]) or by clinical diagnosis (granulomatosis with polyangiitis [GPA] versus microscopic polyangiitis [MPA]).
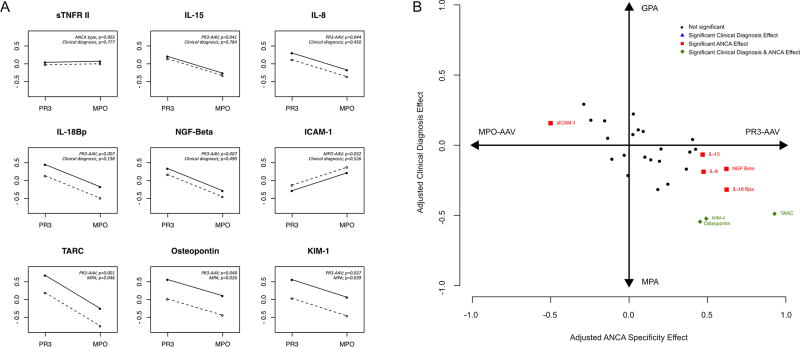
Methods: A panel of 29 cytokines was tested in 186 patients with active AAV at inclusion into the Rituximab in AAV trial. Cytokine concentrations were compared between groups within each classification system. Multivariable analyses adjusted for age, sex, and renal insufficiency were performed, with each biomarker as a dependent variable and ANCA specificity and clinical diagnosis as explanatory variables of interest.
Results: Levels of 9 circulating cytokines (interleukin-6 [IL-6], granulocyte-macrophage colony-stimulating factor [GM-CSF], IL-15, IL-18, CXCL8/IL-8, CCL-17/thymus and activation-regulated chemokine [TARC], IL-18 binding protein [IL-18 BP], soluble IL-2 receptor α [sIL-2Rα], and nerve growth factor β [NGFβ]) were significantly higher in PR3-AAV than MPO-AAV, 4 cytokines (sIL6R, soluble tumor necrosis factor receptor type II [sTNFRII], neutrophil gelatinase-associated lipocalin [NGAL], and soluble intercellular adhesion molecule 1 [sICAM-1]) were higher in MPO-AAV than in PR3-AAV, 6 cytokines (IL-6, GM-CSF, IL-15, IL-18, sIL-2Rα, and NGFβ) were higher in GPA than in MPA, and 3 cytokines (osteopontin, sTNFRII, and NGAL) were higher in MPA than in GPA (all P < 0.05). For nearly all cytokines, the difference between PR3-AAV and MPO-AAV was larger than that between GPA and MPA. The multivariate analysis showed that 8 cytokines (IL-15, IL-8, IL-18 BP, NGF-β, sICAM-1, TARC, osteopontin, and kidney injury molecule 1 (P < 0.05) distinguished patients with AAV better (lower P values and larger effect sizes) when grouped by ANCA specificity than by clinical diagnosis.
Conclusion: Distinct cytokine profiles were identified for PR3-AAV versus MPO-AAV and for GPA versus MPA. Differences in these circulating immune mediators are more strongly associated with ANCA specificity than with clinical diagnosis, suggesting that heterogeneity in the AAV subtypes extends beyond clinical phenotypes.
© 2018, American College of Rheumatology.
Figures
References
-
- Cornec D, Cornec-Le Gall E, Fervenza FC, Specks U. ANCA-associated vasculitis - clinical utility of using ANCA specificity to classify patients. Nature reviews Rheumatology. 2016;12(10):570–9. - PubMed
-
- Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis and rheumatism. 2013;65(1):1–11. - PubMed
-
- Hogan SL, Falk RJ, Chin H, Cai J, Jennette CE, Jennette JC, et al. Predictors of relapse and treatment resistance in antineutrophil cytoplasmic antibody-associated small-vessel vasculitis. Annals of internal medicine. 2005;143(9):621–31. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UL1 RR025005/RR/NCRR NIH HHS/United States
- K23 AR052820/AR/NIAMS NIH HHS/United States
- M01 RR000533/RR/NCRR NIH HHS/United States
- UL1 RR025771/RR/NCRR NIH HHS/United States
- K24 AR002224/AR/NIAMS NIH HHS/United States
- P60 AR047785/AR/NIAMS NIH HHS/United States
- U54 RR019497/RR/NCRR NIH HHS/United States
- U54 NS064808/NS/NINDS NIH HHS/United States
- K24 AR049185/AR/NIAMS NIH HHS/United States
- UL1 RR024150/RR/NCRR NIH HHS/United States
- U54 AR057319/AR/NIAMS NIH HHS/United States
- RC1 AR058303/AR/NIAMS NIH HHS/United States
- N01 AI015416/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
