

Elective induction of labor at 39 weeks among nulliparous women: The impact on maternal and neonatal risk
- PMID: 29694344
- PMCID: PMC5918610
- DOI: 10.1371/journal.pone.0193169
Elective induction of labor at 39 weeks among nulliparous women: The impact on maternal and neonatal risk
Abstract
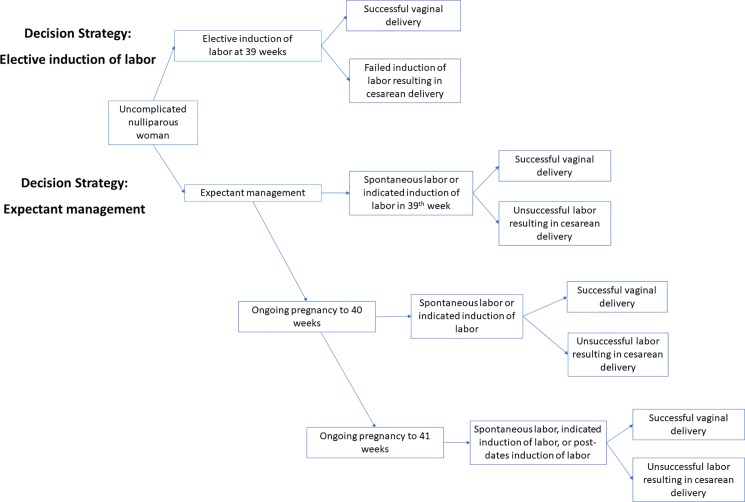
Objective: Optimal management of pregnancies at 39 weeks gestational age is unknown. Therefore, we sought to perform a comparative effectiveness analysis of elective induction of labor (eIOL) at 39 weeks among nulliparous women with non-anomalous singleton, vertex fetuses as compared to expectant management (EM) which included IOL for medical or obstetric indications or at 41 weeks in undelivered mothers.
Materials and methods: A Monte Carlo micro-simulation model was constructed modeling two mutually exclusive health states: eIOL at 39 weeks, or EM with IOL for standard medical or obstetrical indications or at 41 weeks if undelivered. Health state distribution probabilities included maternal and perinatal outcomes and were informed by a review of the literature and data derived from the Consortium of Safe Labor. Analyses investigating preferences for maternal versus infant health were performed using weighted utilities. Primary outcome was determining which management strategy posed less maternal and neonatal risk. Secondary outcomes were rates of cesarean deliveries, maternal morbidity and mortality, stillbirth, neonatal morbidity and mortality, and preferences regarding the importance of maternal and perinatal health.
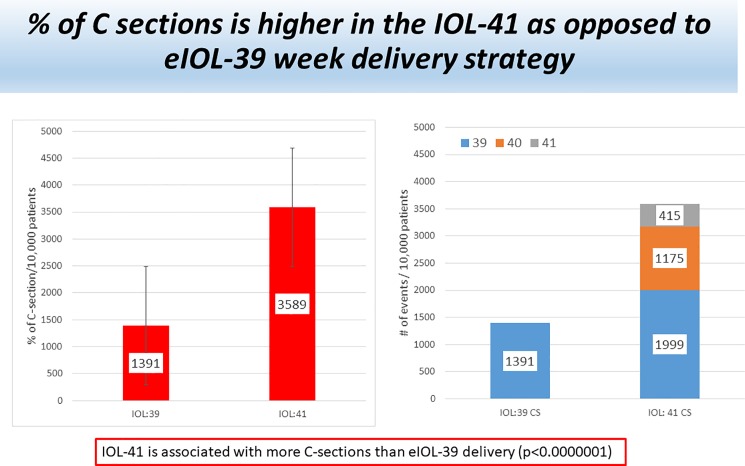
Results: A management strategy of eIOL at 39 weeks resulted in less maternal and neonatal risk as compared to EM with IOL at 41 weeks among undelivered patients. Cesarean section rates were higher in the EM arm (35.9% versus 13.9%, p<0.01). When analysis was performed only on patients with an unfavorable cervix, 39 week eIOL still resulted in fewer cesarean deliveries as compared to EM (8.0% versus 26.1%, p<0.01). There was no statistical difference in maternal mortality (eIOL 0% versus EM 0.01%, p = 0.32) but there was an increase in maternal morbidity among the EM arm (21.2% versus 16.5, p<0.01). There were more stillbirths (0.13% versus 0%, p<0.0003), neonatal deaths (0.25% versus 0.12%, p< 0.03), and neonatal morbidity (12.1% versus 9.4%, p<0.01) in the EM arm as compared to the eIOL arm. Preference modeling revealed that 39 week eIOL was favored over EM.
Conclusions and relevance: Mathematical modeling revealed that eIOL at 39 weeks resulted in lower population risks as compared to EM with induction of labor at 41 weeks. Specifically, eIOL at 39 weeks resulted in a lower cesarean section rate, lower rates of maternal morbidity, fewer stillbirths and neonatal deaths, and lower rates of neonatal morbidity.
Conflict of interest statement
Figures
References
-
- Institute of Medicine Committee on Understanding Premature B, Assuring Healthy O. The National Academies Collection: Reports funded by National Institutes of Health In: Behrman RE, Butler AS, editors. Preterm Birth: Causes, Consequences, and Prevention. Washington (DC): National Academies Press (US) National Academy of Sciences; 2007. - PubMed
-
- Practice bulletin no. 130: prediction and prevention of preterm birth. Obstetrics and gynecology. 2012;120(4):964–73. Epub 2012/09/22. doi: 10.1097/AOG.0b013e3182723b1b . - DOI - PubMed
-
- Practice bulletin no. 146: Management of late-term and postterm pregnancies. Obstetrics and gynecology. 2014;124(2 Pt 1):390–6. Epub 2014/07/23. doi: 10.1097/01.aog.0000452744.06088.48 . - DOI - PubMed
-
- Hilder L, Costeloe K, Thilaganathan B. Prolonged pregnancy: evaluating gestation-specific risks of fetal and infant mortality. British journal of obstetrics and gynaecology. 1998;105(2):169–73. Epub 1998/03/21. . - PubMed
-
- Caughey AB, Stotland NE, Washington AE, Escobar GJ. Maternal and obstetric complications of pregnancy are associated with increasing gestational age at term. American journal of obstetrics and gynecology. 2007;196(2):155.e1–6. Epub 2007/02/20. doi: 10.1016/j.ajog.2006.08.040 ; PubMed Central PMCID: PMCPmc1941614. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
