

Birth Outcomes for Pregnant Women with HIV Using Tenofovir-Emtricitabine
- PMID: 29694825
- PMCID: PMC5984044
- DOI: 10.1056/NEJMoa1701666
Birth Outcomes for Pregnant Women with HIV Using Tenofovir-Emtricitabine
Abstract
Background: In a previous trial of antiretroviral therapy (ART) involving pregnant women with human immunodeficiency virus (HIV) infection, those randomly assigned to receive tenofovir, emtricitabine, and ritonavir-boosted lopinavir (TDF-FTC-LPV/r) had infants at greater risk for very premature birth and death within 14 days after delivery than those assigned to receive zidovudine, lamivudine, and ritonavir-boosted lopinavir (ZDV-3TC-LPV/r).
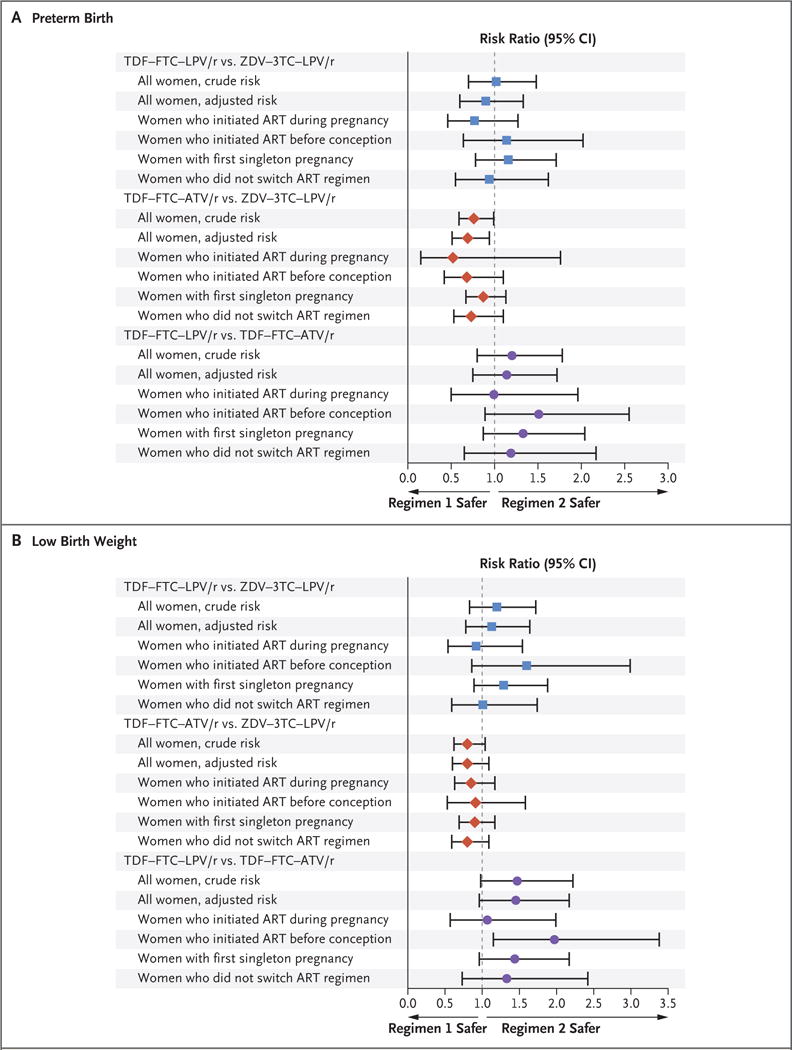
Methods: Using data from two U.S.-based cohort studies, we compared the risk of adverse birth outcomes among infants with in utero exposure to ZDV-3TC-LPV/r, TDF-FTC-LPV/r, or TDF-FTC with ritonavir-boosted atazanavir (ATV/r). We evaluated the risk of preterm birth (<37 completed weeks of gestation), very preterm birth (<34 completed weeks), low birth weight (<2500 g), and very low birth weight (<1500 g). Risk ratios with 95% confidence intervals were estimated with the use of modified Poisson models to adjust for confounding.
Results: There were 4646 birth outcomes. Few infants or fetuses were exposed to TDF-FTC-LPV/r (128 [2.8%]) as the initial ART regimen during gestation, in contrast with TDF-FTC-ATV/r (539 [11.6%]) and ZDV-3TC-LPV/r (954 [20.5%]). As compared with women receiving ZDV-3TC-LPV/r, women receiving TDF-FTC-LPV/r had a similar risk of preterm birth (risk ratio, 0.90; 95% confidence interval [CI], 0.60 to 1.33) and low birth weight (risk ratio, 1.13; 95% CI, 0.78 to 1.64). As compared to women receiving TDF-FTC-ATV/r, women receiving TDF-FTC-LPV/r had a similar or slightly higher risk of preterm birth (risk ratio, 1.14; 95% CI, 0.75 to 1.72) and low birth weight (risk ratio, 1.45; 95% CI, 0.96 to 2.17). There were no significant differences between regimens in the risk of very preterm birth or very low birth weight.
Conclusions: The risk of adverse birth outcomes was not higher with TDF-FTC-LPV/r than with ZDV-3TC-LPV/r or TDF-FTC-ATV/r among HIV-infected women and their infants in the United States, although power was limited for some comparisons. (Funded by the National Institutes of Health and others.).
Figures
References
-
- Cooper ER, Charurat M, Mofenson L, et al. Combination antiretroviral strategies for the treatment of pregnant HIV-1-infected women and prevention of perinatal HIV-1 transmission. J Acquir Immune Defic Syndr. 2002;29:484–94. - PubMed
-
- AIDSinfo. Recommendations for the use of antiretroviral drugs in pregnant women with HIV infection and interventions to reduce perinatal HIV transmission in the United States. Washington, DC: Department of Health and Human Services; 2017. https://aidsinfo.nih.gov/guidelines/html/3/perinatal-guidelines/0.
-
- Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: recommendations for a public health approach. second. Geneva: World Health Organization; 2016. http://www.who.int/hiv/pub/arv/arv-2016/en/ - PubMed
-
- Nurutdinova D, Onen NF, Hayes E, Mondy K, Overton ET. Adverse effects of tenofovir use in HIV-infected pregnant women and their infants. Ann Pharmacother. 2008;42:1581–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials