

Aortic flow patterns and wall shear stress maps by 4D-flow cardiovascular magnetic resonance in the assessment of aortic dilatation in bicuspid aortic valve disease
- PMID: 29695249
- PMCID: PMC5918697
- DOI: 10.1186/s12968-018-0451-1
Aortic flow patterns and wall shear stress maps by 4D-flow cardiovascular magnetic resonance in the assessment of aortic dilatation in bicuspid aortic valve disease
Abstract
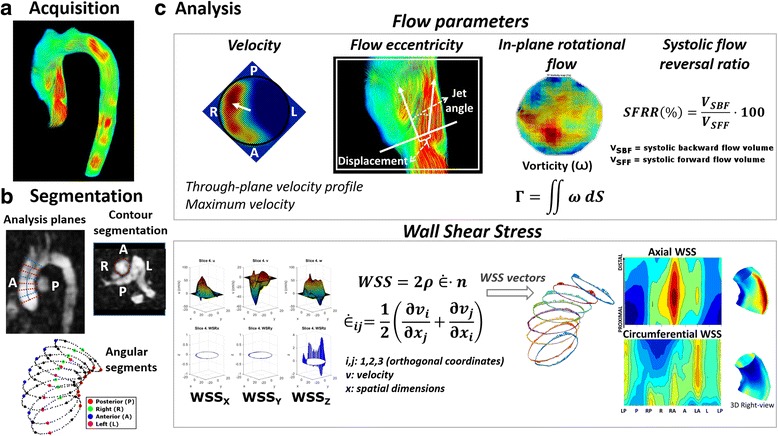
Background: In patients with bicuspid valve (BAV), ascending aorta (AAo) dilatation may be caused by altered flow patterns and wall shear stress (WSS). These differences may explain different aortic dilatation morphotypes. Using 4D-flow cardiovascular magnetic resonance (CMR), we aimed to analyze differences in flow patterns and regional axial and circumferential WSS maps between BAV phenotypes and their correlation with ascending aorta dilatation morphotype.
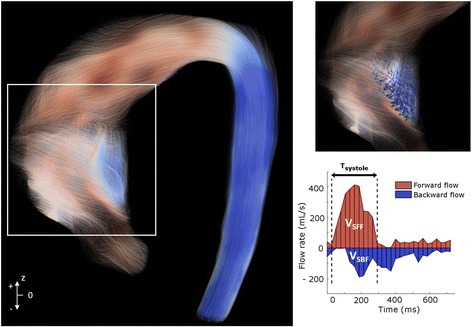
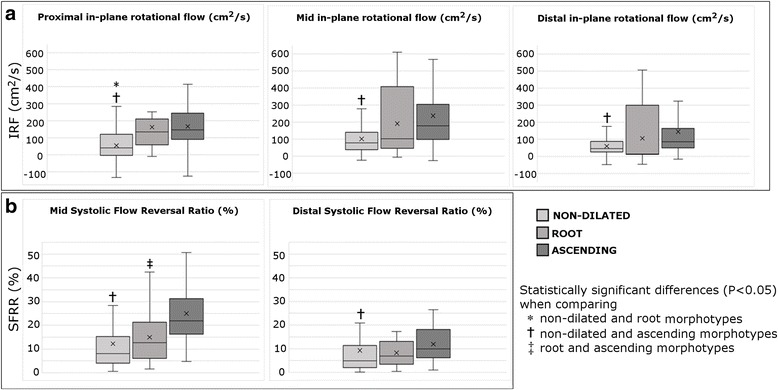
Methods: One hundred and one BAV patients (aortic diameter ≤ 45 mm, no severe valvular disease) and 20 healthy subjects were studied by 4D-flow CMR. Peak velocity, flow jet angle, flow displacement, in-plane rotational flow (IRF) and systolic flow reversal ratio (SFRR) were assessed at different levels of the AAo. Peak-systolic axial and circumferential regional WSS maps were also estimated. Unadjusted and multivariable adjusted linear regression analyses were used to identify independent correlates of aortic root or ascending dilatation. Age, sex, valve morphotype, body surface area, flow derived variables and WSS components were included in the multivariable models.
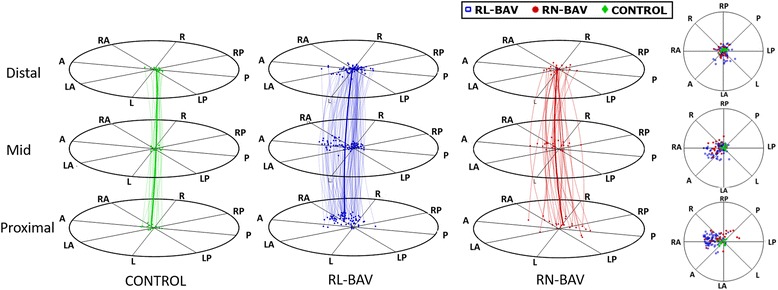
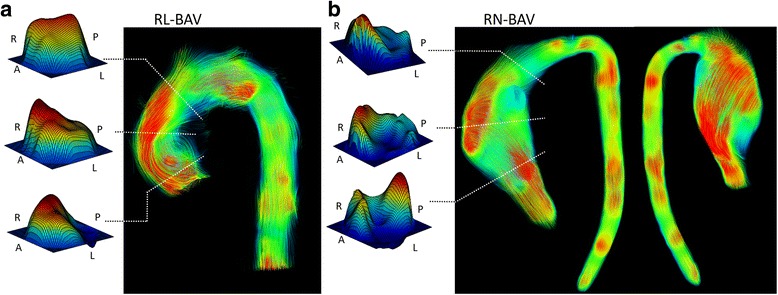
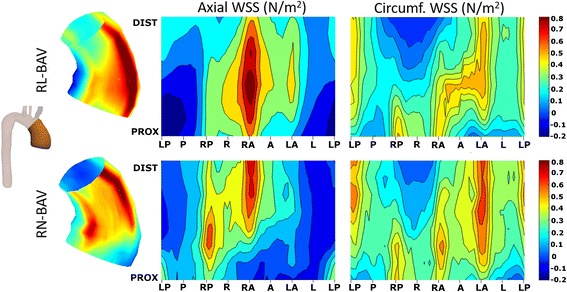
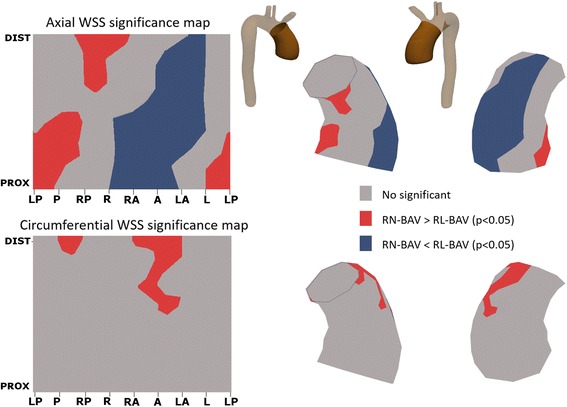
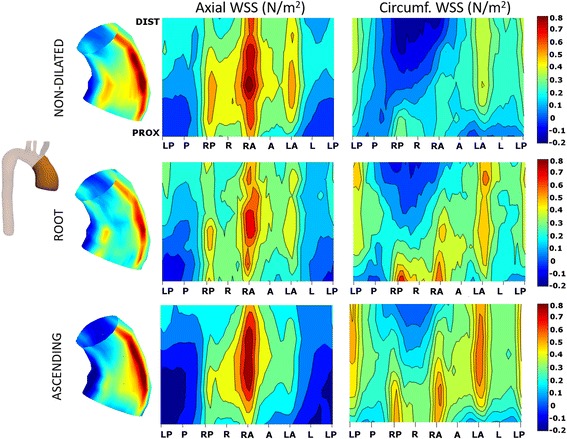
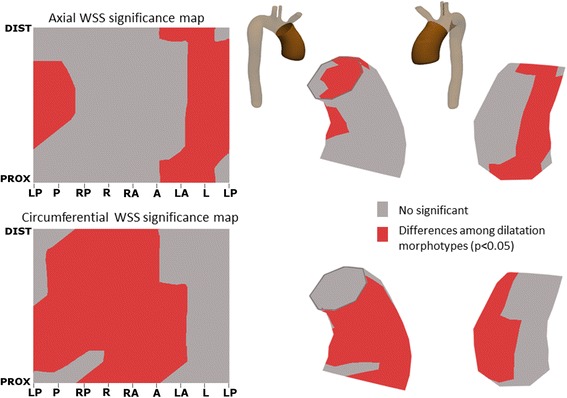
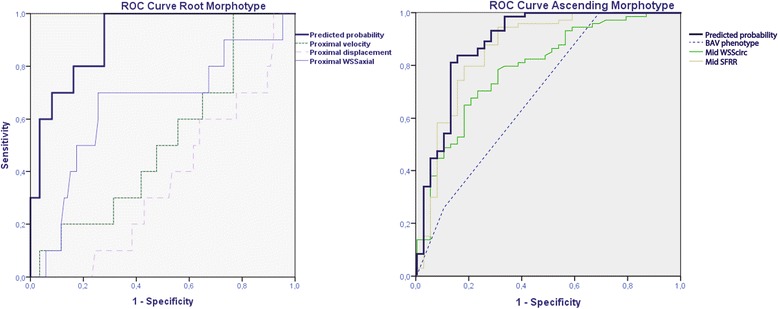
Results: The AAo was non-dilated in 24 BAV patients and dilated in 77 (root morphotype in 11 and ascending in 66). BAV phenotype was right-left (RL-) in 78 patients and right-non-coronary (RN-) in 23. Both BAV phenotypes presented different outflow jet direction and velocity profiles that matched the location of maximum systolic axial WSS. RL-BAV velocity profiles and maximum axial WSS were homogeneously distributed right-anteriorly, however, RN-BAV showed higher variable profiles with a main proximal-posterior distribution shifting anteriorly at mid-distal AAo. Compared to controls, BAV patients presented similar WSS magnitude at proximal, mid and distal AAo (p = 0.764, 0.516 and 0.053, respectively) but lower axial and higher circumferential WSS components (p < 0.001 for both, at all aortic levels). Among BAV patients, RN-BAV presented higher IRF at all levels (p = 0.024 proximal, 0.046 mid and 0.002 distal AAo) and higher circumferential WSS at mid and distal AAo (p = 0.038 and 0.046, respectively) than RL-BAV. However, axial WSS was higher in RL-BAV compared to RN-BAV at proximal and mid AAo (p = 0.046, 0.019, respectively). Displacement and axial WSS were independently associated with the root-morphotype, and circumferential WSS and SFRR with the ascending-morphotype.
Conclusions: Different BAV-phenotypes present different flow patterns with an anterior distribution in RL-BAV, whereas, RN-BAV patients present a predominant posterior outflow jet at the sinotubular junction that shifts to anterior or right anterior in mid and distal AAo. Thus, RL-BAV patients present a higher axial WSS at the aortic root while RN-BAV present a higher circumferential WSS in mid and distal AAo. These results may explain different AAo dilatation morphotypes in the BAV population.
Keywords: 4D flow cardiovascular magnetic resonance (4D flow CMR); Aorta hemodynamics; Aortic dilatation; Ascending aorta; Bicuspid aortic valve; Wall shear stress.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the local ethics committee (Hospital Universitari Vall d’Hebron) and informed consent was obtained from all participants.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Tzemos N, Therrien J, Thanassoulis G, et al. With bicuspid aortic valves. World Health. 2013;300(11):1317–1325. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
