

The influence of the number of screws and additional surgical procedures on outcome in hallux valgus treatment
- PMID: 29695272
- PMCID: PMC5918987
- DOI: 10.1186/s13018-018-0796-z
The influence of the number of screws and additional surgical procedures on outcome in hallux valgus treatment
Abstract
Background: Surgical treatment of hallux valgus (HV) is one of the major flagships of orthopedic surgeons. Due to relatively unsatisfactory radiological and clinical outcomes, the search for the best surgical technique and causes for unsatisfactory outcomes continues. The objective was to investigate associations of the number of screws and additional surgical techniques for HV with radiological and clinical outcome after reversed L-shaped osteotomy (ReveL).
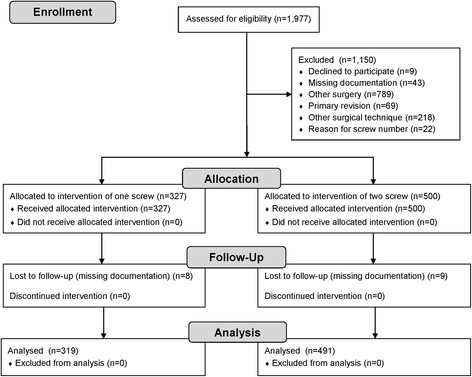
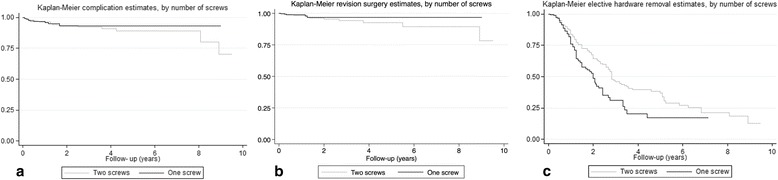
Methods: A retrospective cohort study of adults from a single University Hospital between 2004 and 2013 was performed. The primary exposure was the number of screws (one vs two) used for osseous fixation after ReveL. The secondary exposure was an additional surgical technique for HV (e.g., Akin osteotomy). The primary outcome was a radiological recurrence of HV (HV angle (HVA) > 15°) at last follow-up. The secondary outcomes were limited patient satisfaction, complication, revision surgery, and elective hardware removal. Odds ratio (OR) and 95% confidence interval (CI) were estimated by logistic regression adjusting for confounders.
Results: The recurrence was 45% less likely with the use of one screw, independent of age, sex, additional technique, and preoperative HVA (odds ratio (ORadjusted) = 0.55 [95% CI 0.30-0.98], p = 0.043). The recurrence was 162% more likely with an additional surgical technique for HV (ORadjusted = 2.62 [1.24-5.52], p = 0.011).
Conclusion: In ReveL for HV, a single screw (instead of two screws) may be sufficient enough for a similar or even better outcome, which may also reduce costs. Additional surgical procedures for HV may be refrained from if possible. Due to limitations of a retrospective study, results may need validation with clinical trials.
Keywords: Hallux valgus (HV); Long plantar arm osteotomy; Patient satisfaction; Recurrence; Reversed L-shaped osteotomy (ReveL); Screws.
Conflict of interest statement
Ethics approval and consent to participate
Ethics approval was given by the local ethics committee (cantonal ethics committee Zurich 2015-0480), allowing this retrospective study with a large number of patients to be performed without the need for individually signed informed consent to participate.
Consent for publication
This retrospective study with a large number of patients was allowed by the local ethics committee (cantonal ethics committee Zurich 2015-0480) to be performed without the need for individually signed informed consent for publication.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Austin DW, Leventen EO. A new osteotomy for hallux valgus: a horizontally directed “V” displacement osteotomy of the metatarsal head for hallux valgus and primus varus. Clin Orthop Relat Res. 1981;157:25–30. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
