

Long-term clinical outcomes of cardiac resynchronization therapy with or without defibrillation: impact of the aetiology of cardiomyopathy
- PMID: 29697764
- PMCID: PMC6212789
- DOI: 10.1093/europace/eux357
Long-term clinical outcomes of cardiac resynchronization therapy with or without defibrillation: impact of the aetiology of cardiomyopathy
Abstract
Aims: There is a continuing debate as to whether cardiac resynchronization therapy-defibrillation (CRT-D) is superior to CRT-pacing (CRT-P), particularly in patients with non-ischaemic cardiomyopathy (NICM). We sought to quantify the clinical outcomes after primary prevention of CRT-D and CRT-P and identify whether these differed according to the aetiology of cardiomyopathy.
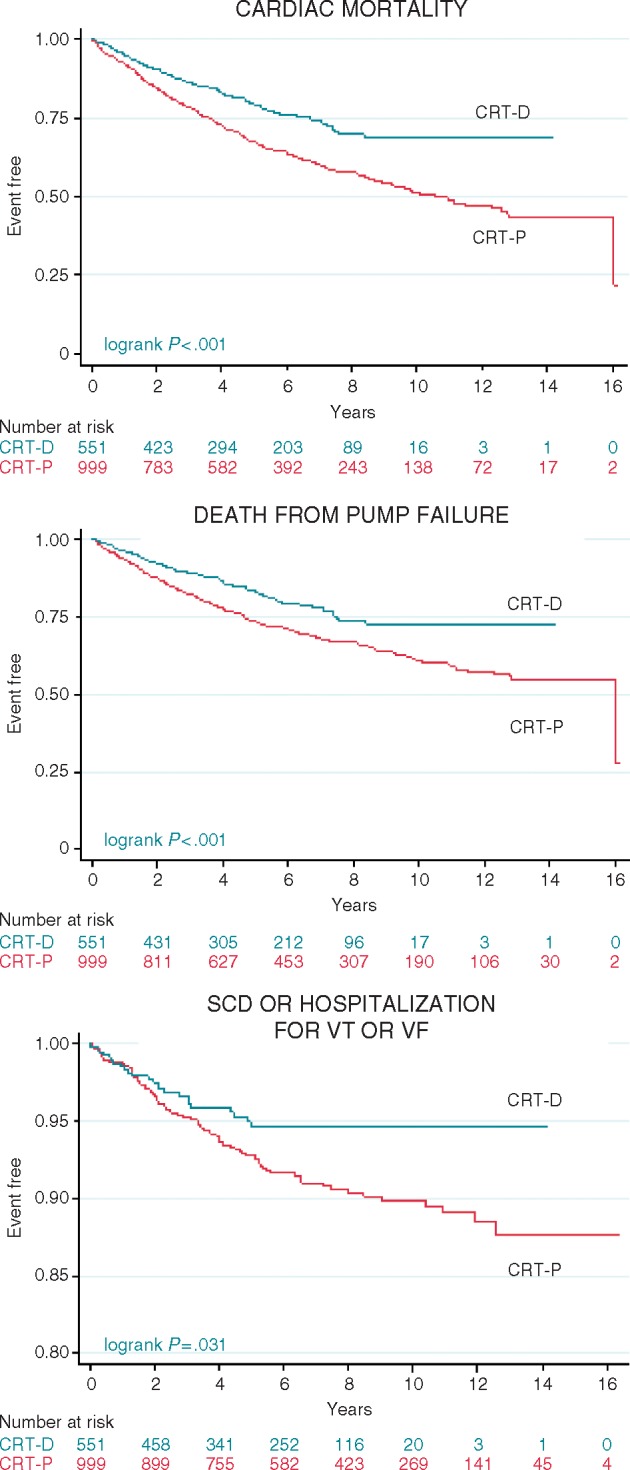
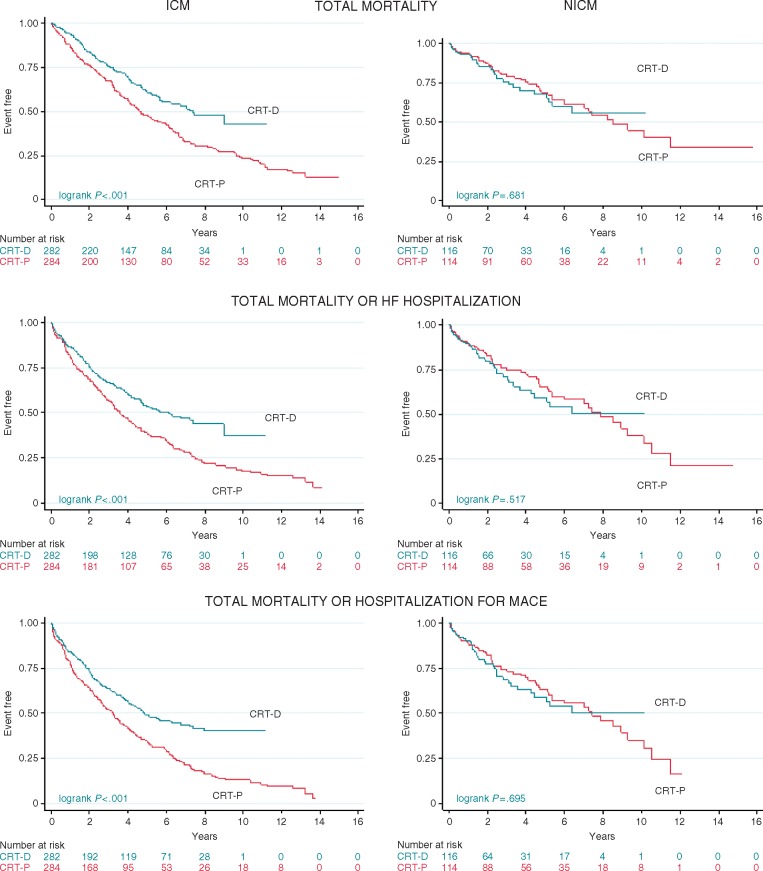
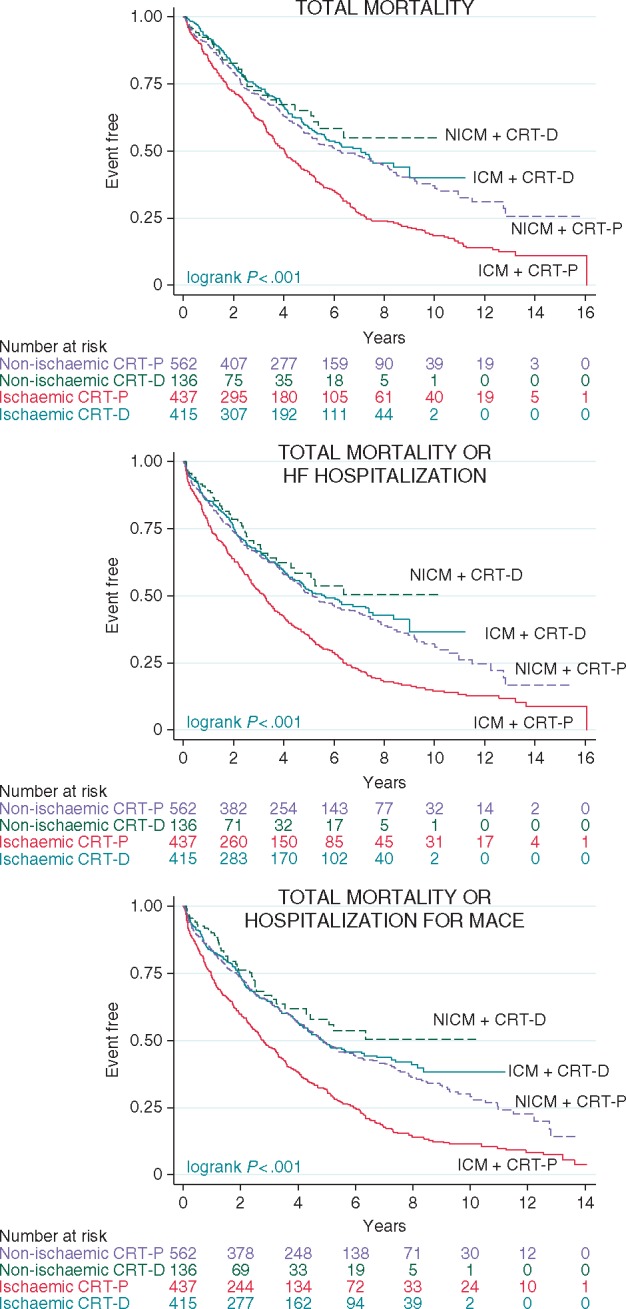
Methods and results: Analyses were undertaken in the total study population of patients treated with CRT-D (n = 551) or CRT-P (n = 999) and in propensity-matched samples. Device choice was governed by the clinical guidelines in the United Kingdom. In univariable analyses of the total study population, for a maximum follow-up of 16 years (median 4.7 years, interquartile range 2.4-7.1), CRT-D was associated with a lower total mortality [hazard ratio (HR) 0.72] and the composite endpoints of total mortality or heart failure (HF) hospitalization (HR 0.72) and total mortality or hospitalization for major adverse cardiac events (MACE; HR 0.71) (all P < 0.001). After propensity matching (n = 796), CRT-D was associated with a lower total mortality (HR 0.72) and the composite endpoints (all P < 0.01). When further stratified according to aetiology, CRT-D was associated with a lower total mortality (HR 0.62), total mortality or HF hospitalization (HR 0.63), and total mortality or hospitalization for MACE (HR 0.59) (all P < 0.001) in patients with ischaemic cardiomyopathy (ICM). There were no differences in outcomes between CRT-D and CRT-P in patients with NICM.
Conclusion: In this study of real-world clinical practice, CRT-D was superior to CRT-P with respect to total mortality and composite endpoints, independent of known confounders. The benefit of CRT-D was evident in ICM but not in NICM.
Figures

Comment in
-
Cardiac resynchronization therapy in heart failure: is the defibrillator needed?Europace. 2018 Nov 1;20(11):1714-1716. doi: 10.1093/europace/euy152. Europace. 2018. PMID: 29947748 No abstract available.
References
-
- Leyva F, Nisam S, Auricchio A.. 20 years of cardiac resynchronization therapy. J Am Coll Cardiol 2014;64:1047–58. - PubMed
-
- Cleland JG, Daubert JC, Erdmann E, Freemantle N, Gras D, Kappenberger L. et al. Longer-term effects of cardiac resynchronization therapy on mortality in heart failure [the CArdiac REsynchronization-Heart Failure (CARE-HF) trial extension phase]. Eur Heart J 2006;27:1928–32. - PubMed
-
- Colquitt J, Mendes D, Clegg A, Harris P, Cooper K, Picot J. et al. Implantable cardioverter defibrillators for the treatment of arrhythmias and cardiac resynchronisation therapy for the treatment of heart failure: systematic review and economic evaluation. Health Technol Assess 2014;18:1. - PMC - PubMed
-
- Cunningham D, Charles R, Cunningham M, Whittaker T.. Cardiac Rhythm Management UK National Clinical Audit Report 2013-2014. London: National Institute for Cardiovascular Outcomes Research; 2013.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
